Articles
- Page Path
- HOME > Epidemiol Health > Volume 45; 2023 > Article
-
Original Article
Associations of breastfeeding duration and the total number of children breastfed with self-reported osteoarthritis in Korea women 50 years and older: a cross-sectional study -
Dajeong Ham1
 , Sanghyuk Bae1,2
, Sanghyuk Bae1,2 -
Epidemiol Health 2023;45:e2023044.
DOI: https://doi.org/10.4178/epih.e2023044
Published online: April 13, 2023
1Department of Preventive Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Environmental Health Center, The Catholic University of Korea, Seoul, Korea
- Correspondence: Sanghyuk Bae Department of Preventive Medicine, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea E-mail: sanghyukb@catholic.ac.kr
© 2023, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,800 Views
- 105 Download
Abstract
-
OBJECTIVES
- Osteoarthritis is the most common joint disease, with a higher prevalence among women than men. The present study aimed to examine the associations of breastfeeding duration and the total number of children breastfed with osteoarthritis in Korean women aged 50 years and older.
-
METHODS
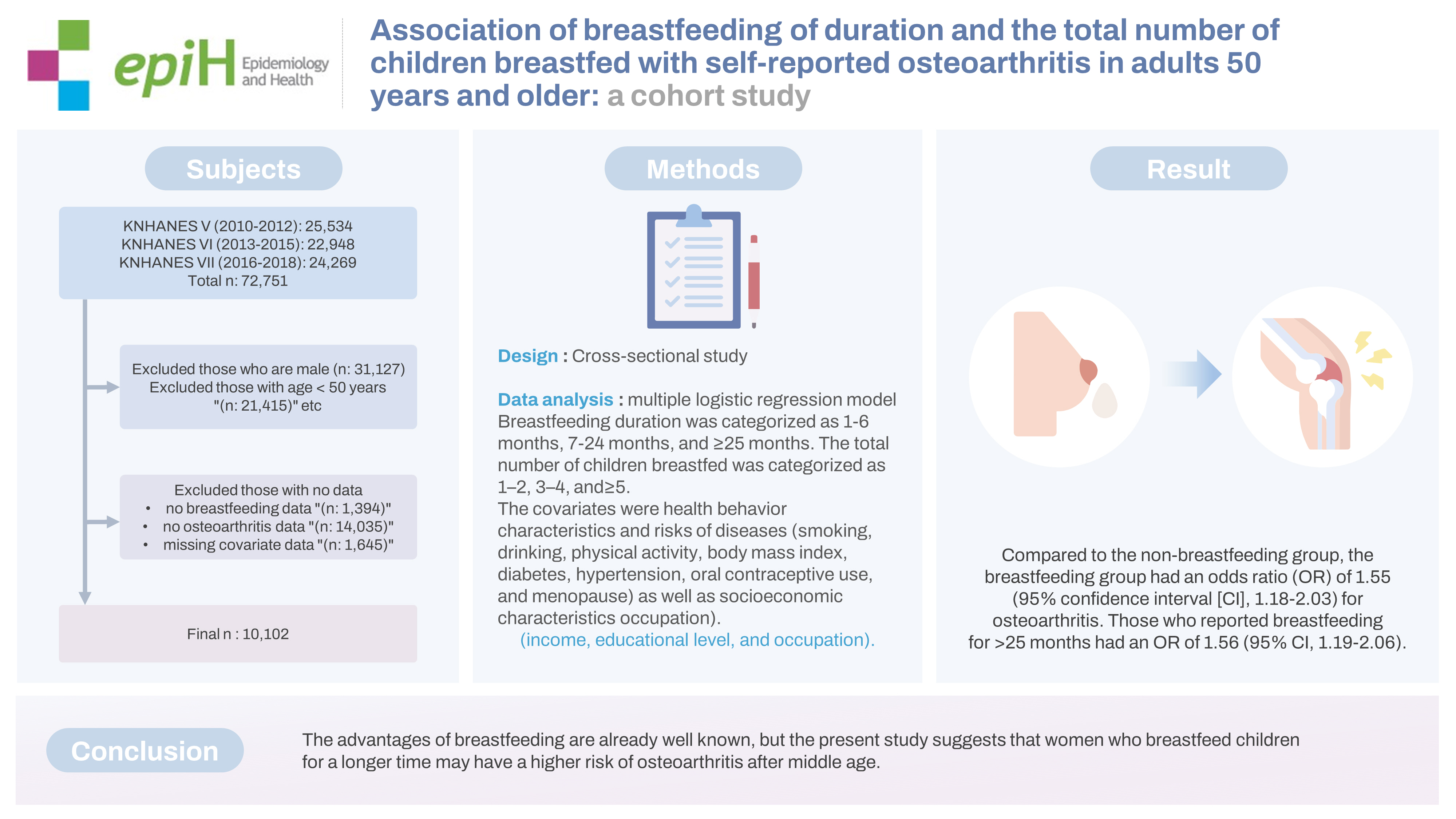
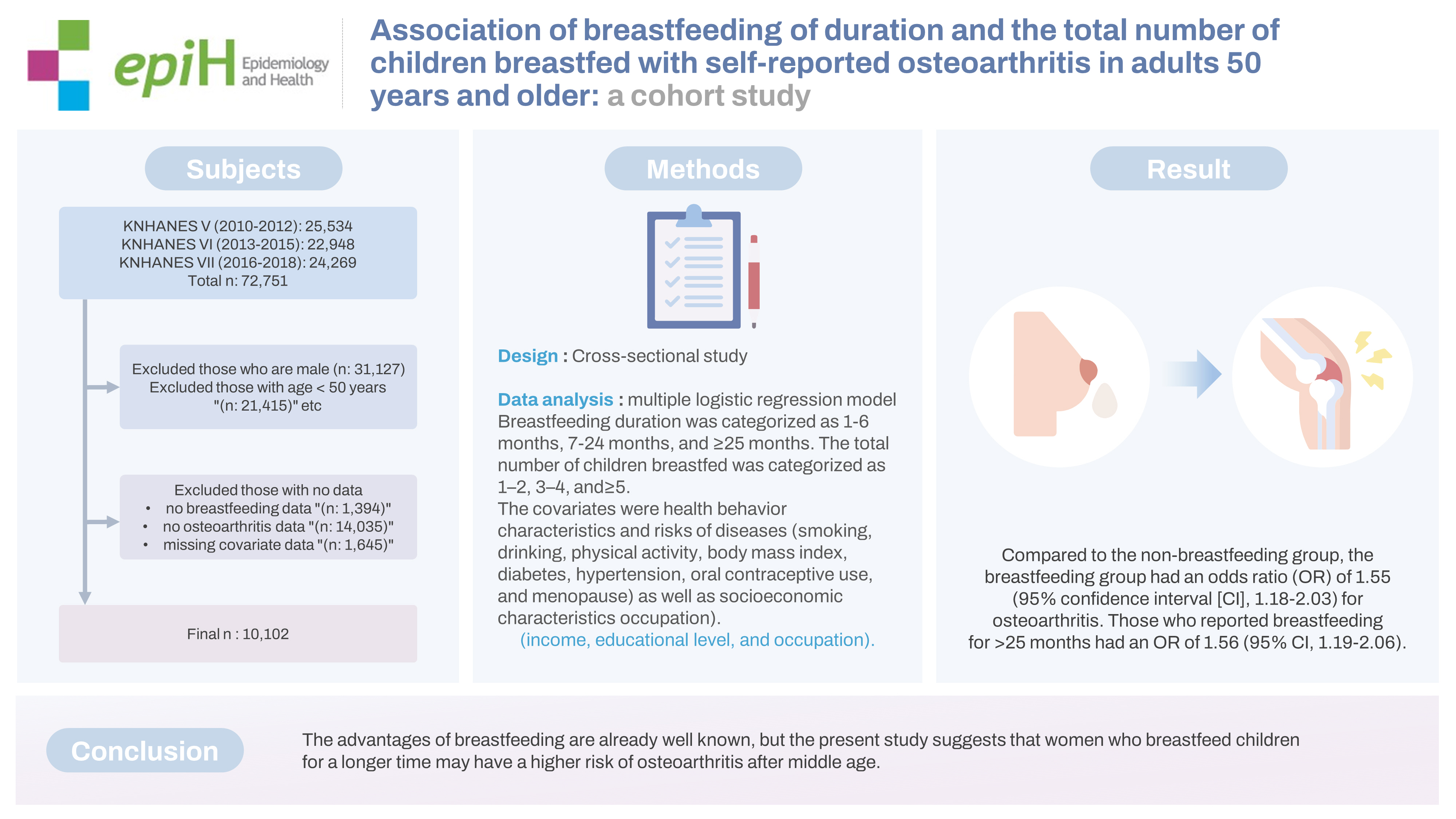
- In this cross-sectional study, we used representative data from the Korea National Health and Nutrition Examination Survey, phases 5 through 7 (2010-2018). Our analysis included 10,102 women aged ≥50 years. Osteoarthritis experience was defined as whether a physician had ever diagnosed osteoarthritis. Breastfeeding duration was categorized as 1-6 months, 7-24 months, and ≥25 months. The total number of children breastfed was categorized as 1-2, 3-4, and ≥5. The covariates were health behavior characteristics and risks of diseases (smoking, drinking, physical activity, body mass index, diabetes, hypertension, oral contraceptive use, and menopause) as well as socioeconomic characteristics (income, educational level, and occupation). A multiple logistic regression model was used to investigate associations between osteoarthritis and aspects of breastfeeding experience.
-
RESULTS
- Compared to the non-breastfeeding group, the breastfeeding group had an odds ratio (OR) of 1.55 (95% confidence interval [CI], 1.18 to 2.03) for osteoarthritis. Those who reported breastfeeding for >25 months had an OR of 1.56 (95% CI, 1.19 to 2.06).
-
CONCLUSIONS
- The advantages of breastfeeding are already well known, but the present study suggests that women who breastfeed children for a longer time may have a higher risk of osteoarthritis after middle age.
- Osteoarthritis is a condition in which the cartilage present in the joints between bones is worn out and the adjacent bone surfaces are exposed, causing inflammation of the membrane surrounding the joint. Osteoarthritis is the most common joint disease [1,2]. Osteoarthritis affects 31% of Korean adults aged 65 years and older [3], and globally, 9.6% of men and 18.0% of women over 60 years of age are affected [2]. As the total number of elderly people increases worldwide, the proportion of affected individuals is expected to increase, and the resulting economic burden for individuals and society is also expected to be high [4,5]. Osteoarthritis has many risk factors, such as age, gender, heredity, body mass index (BMI), smoking, alcohol use, nutrition, hormone levels, bone density, trauma, physical activity, muscle strength, and occupation [5].
- The prevalence of osteoarthritis is higher in women than in men [6,7]. Women experience various hormonal changes due to pregnancy, childbirth, and menopause [8,9], including estrogen deficiency, which may cause bone loss [10-13]. One risk factor affecting hormone levels in women is breastfeeding. Breastfeeding has long-term and short-term benefits for both mother and child [14]. It lowers the maternal risks of obesity, type 1 and 2 diabetes, hypertension, cardiovascular disease, hyperlipidemia, and cancer [14,15]. Breastfeeding also has many psychological benefits, such as a lower chance of maternal depression [16]. For children, it helps their cognitive and social development [16]. However, breastfeeding may also have negative effects such as pain [17], sexual dysfunction [18], and viral infections [19,20]. Recent studies have investigated the risk of subsequent osteoarthritis [21-23].
- Many studies have examined the association between breastfeeding and osteoporosis risk [24-26]. However, evidence for an association between breastfeeding and osteoarthritis is inconsistent, and the association between the number of children breastfed and osteoarthritis has not been studied previously. In an earlier study examining the association between osteoarthritis and menopause, estrogen deficiency after menopause worsened osteoarthritis [26-28]. Additionally, several studies have shown that postmenopausal estrogen replacement therapy can prevent osteoarthritis [26-28]. An earlier study on the association of osteoarthritis with childbirth and lactation found that women aged ≥ 50 years who had breastfed a child for at least one month had a higher risk of developing osteoarthritis than women who had breastfed for less than one month [21]. In contrast, a recent study reported that the number of children and duration of breastfeeding were not associated significantly with osteoarthritis [23]. The inconsistency in results between studies may be due to differences in survey methods, sample selection, number of samples, and analytical methods.
- The present study aimed to analyze the associations of breastfeeding duration and the total number of children breastfed with the prevalence of osteoarthritis in a nationally representative sample of Korea National Health and Nutrition Examination Survey (KNHANES) data, using all available data on breastfeeding duration and the total number of children.
INTRODUCTION
- Study population
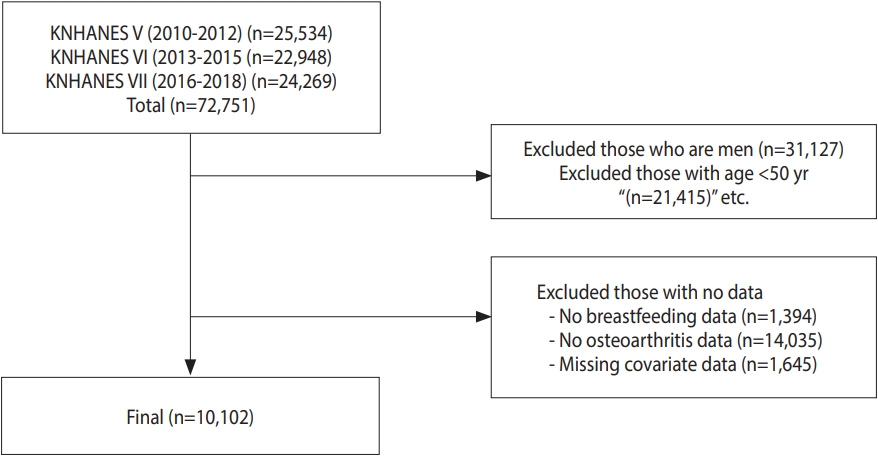
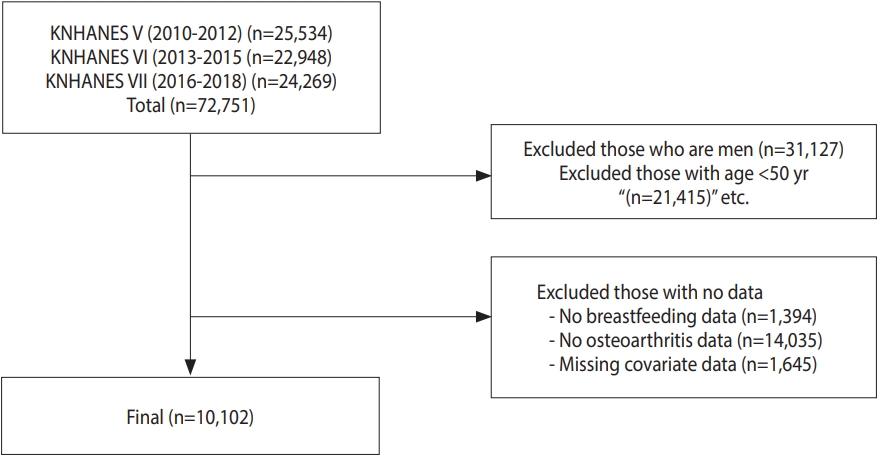
- KNHANES is a nationwide health and nutrition survey conducted by the Korea Disease Control and Prevention Agency. This cross-sectional survey includes approximately 10,000 individuals each year and collects information on socioeconomic conditions, health-related behaviors, quality of life, medical use, human measurements, and biochemical and clinical profiles with three component surveys: health interview, health examination, and nutrition survey. The present study used KNHANES data conducted during the fifth (2010-2012), sixth (2013-2015), and seventh (2016-2018) phases [29].
- The total number of participants in these phases was 72,751. After excluding men, individuals aged < 50 years, and those who had no breastfeeding data, no osteoarthritis data, or missing covariate data, a total of 10,102 women were included in the analyses (Figure 1).
- Outcome measurement
- Participants with osteoarthritis were defined as those who answered “yes” to the question “Have you ever been diagnosed with osteoarthritis?” in the health questionnaire, or those diagnosed by a physician during the survey based on radiological examination of any joint.
- Exposure assessment
- Those with breastfeeding experience were defined as those who answered “yes” to the question “Have you ever breastfed for at least a month?” We also used the answers to the questions “What is the total number of children breastfed?” and “How long was the total period of breastfeeding?” Breastfeeding duration was categorized as 1-6 months, 7-24 months, and ≥ 25 months based on the World Health Organization-recommended periods [30]. The total number of children breastfed was categorized as 1-2, 3-4, and ≥ 5.
- Covariates
- Potential confounding factors were selected a priori from the literature [31,32]. Covariates were also derived from answers to the questionnaire. The socio-demographic covariates were age, income (lowest, medium-low, medium-high, and highest), educational level (elementary, middle school, high school and college), and occupation (professionals and related workers, office workers, service and sales workers, agricultural, forestry and fishery trades, technical workers and machinery operation and assembly workers, manual labor jobs, and unemployed). The health and behavior covariates were defined as smoking status (non-smoking, ex-smoker, and current smoker), physical activity (yes or no), drinking experience (yes or no), BMI (underweight: < 18.5; normal: ≥ 18.5 and < 23.0; pre-obesity: ≥ 23.0 and < 25.0; stage 1 obesity: ≥ 25.0 and < 30.0; and stage 2-3 obesity ≥ 30.0 kg/m2), hypertension (hypertension, pre-hypertension, and normal), diabetes (normal, impaired fasting glucose, and diabetes). Experience with oral contraceptives was measured on the health questionnaire by “Have you taken oral contraceptives for at least 1 month?” (yes or no), and those who answered “natural menopause” or “artificial menopause” were classified as menopausal, whereas those who answered “menstrual period,” “pregnancy,” or “lactating after childbirth” were classified as non-menopausal. Parity was measured from the number of total pregnancies from the health questionnaire.
- Statistical analysis
- KNHANES uses stratified cluster sampling with weights. Therefore, the statistical analysis was conducted using composite sample data that accounted for sampling weights. For categorical variables, data were presented as frequencies and percentages, and the chi-square test was used for comparisons. For continuous variables, data were presented as mean and standard deviation, and analysis of variance was used for comparisons. In the main analysis, a multiple logistic regression model was used to examine the associations of breastfeeding duration and the number of breastfed children with self-reported osteoarthritis. We adjusted for potential confounders: in model 1, we adjusted only for age; in model 2, we additionally adjusted for health and behavior covariates (smoking experience, drinking experience, physical activity, BMI, diabetes, hypertension, use of oral contraceptives, and menopause); and in model 3, we additionally adjusted for socioeconomical covariates (income level, educational level, and occupation). Due to the high prevalence of osteoarthritis in the elderly, subgroup analyses were conducted and stratified by age in years: 50s, 60s, and 70s or older. Since data on osteoarthritis prevalence were collected by 2 methods during part of KNHANES (fifth and sixth phases, conducted in 2010-2013)−namely, a self-administered questionnaire and radiological findings—a sensitivity analysis was conducted to investigate whether these 2 methods yielded different results. Odds ratios (ORs) and 95% confidence intervals (CIs) were presented. The Cochran-Armitage trend test was used to analyze trends in breastfeeding duration and the number of breastfed children. Multicollinearity was tested by the variance inflation factor (VIF).
- Ethics statement
- The protocol of the present study was approved by the Institutional Review Board at The Catholic University of Korea (MC20ZASI0133).
MATERIALS AND METHODS
- Table 1 shows the general characteristics of the participants. Women with breastfeeding experience were generally older and reported lower income and educational levels than those who reported no breastfeeding experience. Those with longer breastfeeding periods were more likely to report lower educational levels, diabetes, and high blood pressure.
- Table 2 shows the association between breastfeeding duration and osteoarthritis. After adjusting for potential confounders, the group with breastfeeding experience had an OR of 1.55 (95% CI, 1.18 to 2.03) compared to the non-breastfeeding group. The associations were similar according to the breastfeeding duration (p for trend < 0.001). The number of breastfed children was also associated significantly with osteoarthritis (p for trend < 0.001). Compared to the non-breastfeeding group, the group that had breastfed 3 or 4 children had an OR of 1.37 (95% CI, 1.10 to 1.71), and the group that had breastfed 5 or more children had an OR of 1.55 (95% CI, 1.18 to 2.03) (Table 3).
- Age-stratified analysis showed no significant association among women in their 50s. However, for those in their 60s or ≥ 70 years of age, the associations were significant for breastfeeding experience lasting 1-6 months (Table 4). Among those ≥ 50 years, the OR was 1.53 (95% CI, 1.07 to 2.21) for those who had breastfed 3 or 4 children. For participants who had breastfed 5 or more children, those in their 60s had an OR of 2.04 (95% CI, 1.24 to 3.35), and those aged 70s and older had an OR of 1.96 (95% CI, 1.19 to 3.23) (Table 5).
- Supplementary Material 1 shows the VIF from the regression analysis. All variables had a VIF < 10. Results of subgroup analyses with radiologically diagnosed osteoarthritis showed a similar pattern (Supplementary Materials 2-5).
RESULTS
- In the present study, breastfeeding experience was associated with a higher prevalence of osteoarthritis among women aged ≥ 50 years in the nationally representative survey in Korea. Compared to the non-breastfeeding group, the breastfeeding group had an OR of 1.55 (95% CI, 1.18 to 2.03) for osteoarthritis. After adjusting for the number of children breastfed, those who reported a breastfeeding duration of > 25 months showed a significant association with osteoarthritis (OR, 1.56; 95% CI, 1.19 to 2.06). That is, participants were more likely to have osteoarthritis the longer they had breastfed, regardless of the number of children. This finding is important because the number of children breastfed was also significantly associated with osteoarthritis (OR, 1.37; 95% CI, 1.10 to 1.71 for 3-4 children and OR, 1.55; 95% CI, 1.18 to 2.03 for 5 or more children, respectively).
- American women over 50 years of age with a history of breastfeeding were found to have a higher risk of developing osteoarthritis than women who did not breastfeed (OR, 1.21; 95% CI, 1.05 to 1.40) [21]. Among Korean women over 50 years of age, the prevalence of knee osteoarthritis diagnosed radiologically among those who had breastfed for 25-48 months was higher than that among non-breastfeeding women (OR, 2.30; 95% CI, 1.09 to 4.86); for those with a breastfeeding duration of more than 48 months, the prevalence of knee osteoarthritis was higher than that in non-breastfeeding women (OR, 2.17; 95% CI, 1.01 to 4.64) [22]. In a study using Women’s Health Initiative data, among postmenopausal women aged ≥ 50 years, those who had breastfed for 1-3 months (OR, 1.026; 95% CI, 1.017 to 1.034) or 4-6 months (OR, 1.015; 95% CI, 1.006 to 1.025) were more likely to self-report osteoarthritis than those who had never breastfed [23]. We found no studies examining the association between the number of children breastfed and osteoarthritis. The present study provides additional evidence on the association between breastfeeding and self-reported osteoarthritis in any joint.
- Women hormones may explain the underlying mechanism supporting the present study’s findings. Estrogen increases during pregnancy and temporarily decreases postpartum, including during lactation [8,9], with a further decrease after menopause. Estrogen deficiency can affect collagen synthesis, bone density, and maintenance of chondrocytes [10,11,27]. Bone loss through estrogen deficiency is due to the complex interaction of hormones and cytokines that interfere with the bone remodeling process. Estrogen inhibits the activity of T cells by inhibiting interleukin-7 and interferon-γ production in the bone marrow, thymus, and peripheral lymphoid organs, and it acts to suppress the production of tumor necrosis factor, a factor that also stimulates osteoclast production. However, estrogen deficiency results in an imbalance in the production-inhibition system of these factors, exacerbating bone loss [12]. In fact, according to a study that confirmed the risk of developing osteoarthritis by measuring the concentration of major estrogen metabolites through a urine test before osteoarthritis was assessed and diagnosed, the risk of osteoarthritis of the knee is high if the concentration of estrogen metabolites is low [33].
- Breastfeeding has many advantages and is recommended. It reduces the risks of developing breast cancer, ovarian cancer, and type 1 and 2 diabetes, and it extends the duration of postpartum infertility [14-16,34]. However, the current study shows that women who have breastfed for a long time and have breastfed many children may be at higher risk for osteoarthritis. In other words, although breastfeeding is not a direct cause of osteoarthritis, extended periods of lactation may be more likely to lead to osteoarthritis, regardless of the specific pathway. Therefore, caution is needed regarding osteoarthritis management (weight control, early screening, etc.) in this population.
- The present study has several limitations. First, the cross-sectional study design prevents inferring causality between breastfeeding and osteoarthritis. The results of this study present a noncausal association, which may be useful for identifying individuals at higher risk. Second, because a questionnaire was used to assess exposure, recall bias is possible. In particular, for older participants, more time is likely to have passed between their experiences of breastfeeding and the survey. Although we observed similar associations in analyses stratified by age, recall bias remains possible within strata. Among the variables used for analysis, osteoarthritis is usually diagnosed by comprehensively considering radiological findings, physical examination, and past history. Although a recent study using KNHANES noted minimal overlap between radiographically diagnosed and self-reported osteoarthritis [35], KNHANES has a quality-control program to manage measurement errors such as estimation and recall problems and interviewer mistakes [36]. Furthermore, questionnaires are widely recognized in health research as a useful tool to gather information on behaviors such as smoking and exercise. Third, osteoarthritis is a disease that occurs in specific parts of the body, such as knees, hips, spine, and fingers. However, because the KNHANES questionnaire for self-reported osteoarthritis does not collect data on which joint(s) may be affected, this aspect could not be analyzed. Fourth, breastfeeding may involve varying amounts and methods, such as single feeding and mixed feeding. Because KNHANES does not contain the relevant data, we could not analyze the effects of different breastfeeding methods.
- The advantages of breastfeeding are well known, but the present study suggests that women who have breastfed for longer periods may have a higher risk of developing osteoarthritis after middle age. An individual’s breastfeeding history may be used to evaluate the risk of osteoarthritis.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Material 1.
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
Supplementary Material 5
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
None.
-
AUTHOR CONTRIBUTIONS
Both authors contributed equally to conceiving the study, analyzing the data, and writing this paper.
NOTES
ACKNOWLEDGEMENTS
| Characteristics | All (n=10,102) |
Breastfeeding experience (mo) |
p value1 | ||||
|---|---|---|---|---|---|---|---|
| None (n=965) | 1-6 (n=754) | 7-24 (n=3,120) | ≥25 (n=5,263) | ||||
| Age (yr) | 62.7±0.1 | 57.7±0.3 | 56.6±0.2 | 58.7±0.1 | 67.8±0.2 | <0.001 | |
| Income | |||||||
| Lowest | 2,354 (23.3) | 188 (2.1) | 134 (1.4) | 671 (7.0) | 1,361 (12.6) | <0.001 | |
| Medium-low | 2,527 (25.1) | 230 (2.7) | 173 (1.8) | 749 (8.2) | 1,375 (12.3) | ||
| Medium-high | 2,571 (25.4) | 251 (2.7) | 171 (2.0) | 840 (9.0) | 1,309 (11.5) | ||
| Highest | 2,650 (26.1) | 296 (3.1) | 276 (2.9) | 860 (9.0) | 1,218 (10.9) | ||
| Educational level | |||||||
| Elementary | 5,098 (46.2) | 225 (2.1) | 118 (1.2) | 939 (9.4) | 2,342 (80.8) | <0.001 | |
| Middle school | 1,674 (17.3) | 114 (1.4) | 106 (1.1) | 698 (7.5) | 3,816 (33.4) | ||
| High school | 2,302 (25.3) | 343 (4.0) | 304 (3.4) | 1,106 (12.4) | 756 (7.2) | ||
| College | 1,028 (10.9) | 283 (3.2) | 226 (2.5) | 377 (3.8) | 549 (5.4) | ||
| Occupation | <0.001 | ||||||
| Managers & specialists | 345 (3.7) | 84 (0.9) | 83 (0.9) | 126 (1.3) | 52 (0.4) | ||
| Clerks | 256 (2.8) | 63 (0.6) | 45 (0.5) | 103 (1.2) | 45 (0.4) | ||
| Sales workers | 1,462 (16.2) | 153 (1.7) | 142 (1.6) | 656 (7.5) | 511 (5.2) | ||
| Agricultural, forestry, & fishery workers | 690 (5.6) | 19 (0.1) | 10 (0.1) | 114 (1.0) | 547 (4.3) | ||
| Engineers & technicians | 260 (2.7) | 23 (0.2) | 27 (0.3) | 127 (1.3) | 83 (0.7) | ||
| Manual laborers | 1,378 (14.2) | 129 (1.4) | 79 (0.9) | 436 (4.8) | 734 (6.9) | ||
| None | 5,711 (54.4) | 494 (5.4) | 368 (3.8) | 1,558 (16.0) | 3,291 (29.1) | ||
| Smoking status | <0.001 | ||||||
| Non-smoking | 9,572 (94.4) | 875 (9.8) | 697 (7.6) | 2,960 (31.5) | 5,040 (45.3) | ||
| Ex-smoker | 231 (2.2) | 47 (0.5) | 24 (0.2) | 63 (0.6) | 97 (0.8) | ||
| Current smoker | 299 (3.2) | 43 (0.4) | 33 (0.4) | 97 (1.0) | 126 (1.2) | ||
| Physical activity | <0.001 | ||||||
| Yes | 8,196 (80.5) | 738 (8.2) | 550 (6.0) | 2,410 (25.4) | 4,498 (40.7) | ||
| No | 1,906 (19.4) | 227 (2.5) | 204 (2.2) | 710 (7.8) | 765 (6.7) | ||
| Drinking experience | <0.001 | ||||||
| Yes | 2,810 (25.9) | 228 (2.4) | 126 (1.2) | 651 (6.2) | 1,805 (15.9) | ||
| Not obese | 7,292 (74.1) | 737 (8.3) | 628 (7.0) | 2,469 (27.0) | 3,458 (31.5) | ||
| Body mass index | <0.001 | ||||||
| Underweight | 175 (1.8) | 32 (0.3) | 19 (0.2) | 50 (0.5) | 74 (0.6) | ||
| Normal | 3,467 (35.3) | 427 (4.9) | 349 (3.9) | 1,175 (12.7) | 1,516 (13.7) | ||
| Pre-obesity | 2,568 (24.8) | 242 (2.6) | 178 (1.8) | 801 (8.4) | 1,347 (11.8) | ||
| Stage 1 obesity | 3,334 (32.6) | 226 (2.4) | 177 (1.9) | 939 (10.0) | 1,992 (18.1) | ||
| Stage 2-3 obesity | 558 (5.3) | 38 (0.4) | 31 (0.3) | 155 (1.6) | 334 (3.0) | ||
| Diabetes | <0.001 | ||||||
| Normal | 5,793 (57.7) | 590 (6.6) | 509 (5.5) | 1,962 (21.2) | 2,732 (24.2) | ||
| IFG | 2,597 (25.9) | 253 (2.7) | 164 (1.8) | 779 (8.5) | 1,401 (12.7) | ||
| Diabetes | 1,712 (16.2) | 122 (1.4) | 81 (0.9) | 379 (3.5) | 1,130 (10.3) | ||
| Hypertension | <0.001 | ||||||
| Normal | 2,850 (30.9) | 376 (4.5) | 325 (3.6) | 1,117 (12.6) | 1,032 (10.0) | ||
| Pre-hypertension | 2,304 (23.2) | 237 (2.6) | 199 (2.2) | 778 (8.4) | 1,090 (9.8) | ||
| Hypertension | 4,948 (45.7) | 352 (3.5) | 230 (2.4) | 1,225 (12.2) | 3,141 (27.5) | ||
| Oral contraceptive experience | <0.001 | ||||||
| Yes | 2,291 (21.7) | 140 (1.6) | 116 (1.1) | 633 (6.4) | 1,402 (12.4) | ||
| No | 7,811 (78.2) | 825 (9.1) | 638 (7.1) | 2,487 (26.8) | 3,861 (35.0) | ||
| Menopause status | <0.001 | ||||||
| Yes | 612 (7.7) | 138 (1.7) | 124 (1.6) | 248 (3.1) | 102 (1.2) | ||
| No | 9,490 (92.2) | 827 (9.0) | 630 (6.7) | 2,872 (30.2) | 5,161 (46.2) | ||
| Parity | 4.50±0.02 | 3.40±0.05 | 3.60±0.07 | 3.80±0.03 | 3.50±0.03 | ||
Values are presented as odds ratio (95% confidence interval).
1 Model 1 was adjusted for age; Model 2 was adjusted for age, body mass index, smoking status, drinking experience, physical activity, diabetes, hypertension, use of oral contraceptives, menopause status, total number of children breastfed, and parity; Model 3 was adjusted for age, income, educational level, occupation, body mass index, smoking status, drinking experience, physical activity, diabetes, hypertension, use of oral contraceptives, menopause status, total number of children breastfed, and parity.
Values are presented as odds ratio (95% confidence interval).
1 Model 1 was adjusted for age; Model 2 was adjusted for age, body mass index, smoking status, drinking experience, physical activity, diabetes, hypertension, use of oral contraceptives, menopause status, and parity; Model 3 was adjusted for age, income, educational level, occupation, body mass index, smoking status, drinking experience, physical activity, diabetes, hypertension, use of oral contraceptives, menopause status, and parity.
Values are presented as odds ratio (95% confidence interval).
1 Adjusted for income, education level, occupation, body mass index, smoking status, drinking experience, physical activity, diabetes, hypertension, use of oral contraceptives, menopause status, total number of children breastfed, and parity.
- 1. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ 2003;81:646-656.PubMedPMC
- 2. Glyn-Jones S, Palmer AJ, Agricola R, Price AJ, Vincent TL, Weinans H, et al. Osteoarthritis. Lancet 2015;386:376-387.ArticlePubMed
- 3. Korea Disease Control and Prevention Agency. Korea health statistics 2019: Korea National Health and Nutrition Examination Survey (KNHANES VIII-1); 2020 [cited 2022 Jun 30]. Available from: https://knhanes.kdca.go.kr/knhanes/main.do (Korean).
- 4. Hunter DJ, Schofield D, Callander E. The individual and socioeconomic impact of osteoarthritis. Nat Rev Rheumatol 2014;10:437-441.ArticlePubMedPDF
- 5. O’Neill TW, McCabe PS, McBeth J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract Res Clin Rheumatol 2018;32:312-326.ArticlePubMed
- 6. Srikanth VK, Fryer JL, Zhai G, Winzenberg TM, Hosmer D, Jones G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthritis Cartilage 2005;13:769-781.ArticlePubMed
- 7. Hame SL, Alexander RA. Knee osteoarthritis in women. Curr Rev Musculoskelet Med 2013;6:182-187.ArticlePubMedPMCPDF
- 8. Battin DA, Marrs RP, Fleiss PM, Mishell DR Jr. Effect of suckling on serum prolactin, luteinizing hormone, follicle-stimulating hormone, and estradiol during prolonged lactation. Obstet Gynecol 1985;65:785-788.PubMed
- 9. Tal R, Taylor HS. Endocrinology of pregnancy. In: Feingold KR, Anawalt B, Boyce A, Chrousos G, de Herder WW, Dhatariya K, et al., editors. Endotext. South Dartmouth: MDText.com, Inc.; 2021, p. 4.
- 10. Väänänen HK, Härkönen PL. Estrogen and bone metabolism. Maturitas 1996;23 Suppl:S65-S69.PubMed
- 11. Klein-Nulend J, van Oers RF, Bakker AD, Bacabac RG. Bone cell mechanosensitivity, estrogen deficiency, and osteoporosis. J Biomech 2015;48:855-865.ArticlePubMed
- 12. Weitzmann MN, Pacifici R. Estrogen deficiency and bone loss: an inflammatory tale. J Clin Invest 2006;116:1186-1194.ArticlePubMedPMC
- 13. Seo E, Lee Y, Kim HC. Association between parity and low bone density among postmenopausal Korean women. J Prev Med Public Health 2021;54:284-292.ArticlePubMedPMCPDF
- 14. Binns C, Lee M, Low WY. The long-term public health benefits of breastfeeding. Asia Pac J Public Health 2016;28:7-14.ArticlePubMedPDF
- 15. Chowdhury R, Sinha B, Sankar MJ, Taneja S, Bhandari N, Rollins N, et al. Breastfeeding and maternal health outcomes: a systematic review and meta-analysis. Acta Paediatr 2015;104:96-113.ArticlePubMedPMC
- 16. Krol KM, Grossmann T. Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2018;61:977-985.ArticlePubMedPMCPDF
- 17. Berens PD. Breast pain: engorgement, nipple pain, and mastitis. Clin Obstet Gynecol 2015;58:902-914.PubMed
- 18. Szöllősi K, Szabó L. The association between infant feeding methods and female sexual dysfunctions. Breastfeed Med 2021;16:93-99.ArticlePubMed
- 19. Petrova M, Kamburov V. Breastfeeding and chronic HBV infection: clinical and social implications. World J Gastroenterol 2010;16:5042-5046.ArticlePubMedPMC
- 20. Prendergast AJ, Goga AE, Waitt C, Gessain A, Taylor GP, Rollins N, et al. Transmission of CMV, HTLV-1, and HIV through breastmilk. Lancet Child Adolesc Health 2019;3:264-273.ArticlePubMed
- 21. Park CY. Breastfeeding for one month or longer is associated with higher risk of osteoarthritis in older adults: NHANES 1999-2012. Clin Nutr Res 2017;6:277-284.ArticlePubMedPMCPDF
- 22. Kim MY, Kim HJ, Noh JH, Kim SA, Hwang DS, Lee CH, et al. Relationship of breastfeeding duration with joint pain and knee osteoarthritis in middle-aged Korean women: a cross-sectional study using the Korea National Health and Nutrition Examination Survey. BMC Womens Health 2020;20:213.ArticlePubMedPMCPDF
- 23. Wang A, Zawadzki N, Hedlin H, LeBlanc E, Budrys N, Van Horn L, et al. Reproductive history and osteoarthritis in the Women’s Health Initiative. Scand J Rheumatol 2021;50:58-67.ArticlePubMed
- 24. de Bakker CM, Burt LA, Gabel L, Hanley DA, Boyd SK. Associations between breastfeeding history and early postmenopausal bone loss. Calcif Tissue Int 2020;106:264-273.ArticlePubMedPDF
- 25. Hwang IR, Choi YK, Lee WK, Kim JG, Lee IK, Kim SW, et al. Association between prolonged breastfeeding and bone mineral density and osteoporosis in postmenopausal women: KNHANES 2010-2011. Osteoporos Int 2016;27:257-265.ArticlePubMedPDF
- 26. Sioka C, Fotopoulos A. Parity, breastfeeding, and osteoporosis. Calcif Tissue Int 2021;108:277-278.ArticlePubMedPDF
- 27. Roman-Blas JA, Castañeda S, Largo R, Herrero-Beaumont G. Osteoarthritis associated with estrogen deficiency. Arthritis Res Ther 2009;11:241.ArticlePubMedPMC
- 28. Zhang Y, McAlindon TE, Hannan MT, Chaisson CE, Klein R, Wilson PW, et al. Estrogen replacement therapy and worsening of radiographic knee osteoarthritis: the Framingham Study. Arthritis Rheum 1998;41:1867-1873.ArticlePubMed
- 29. Kweon S, Kim Y, Jang MJ, Kim Y, Kim K, Choi S, et al. Data resource profile: the Korea National Health and Nutrition Examination Survey (KNHANES). Int J Epidemiol 2014;43:69-77.ArticlePubMedPMC
- 30. World Health Organization. Global strategy for infant and young child feeding; 2003 [cited 2023 Jul 19]. Available from: https://www.who.int/publications/i/item/9241562218.
- 31. Johnson VL, Hunter DJ. The epidemiology of osteoarthritis. Best Pract Res Clin Rheumatol 2014;28:5-15.ArticlePubMed
- 32. Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM, et al. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med 2000;133:635-646.ArticlePubMed
- 33. Sowers MR, McConnell D, Jannausch M, Buyuktur AG, Hochberg M, Jamadar DA. Estradiol and its metabolites and their association with knee osteoarthritis. Arthritis Rheum 2006;54:2481-7.ArticlePubMed
- 34. Allen J, Hector D. Benefits of breastfeeding. N S W Public Health Bull 2005;16:42-46.ArticlePubMed
- 35. Kim S, Lee GW, Park CY. Older Korean men with inadequate vitamin D status have lower odds of radiologic osteoarthritis. Sci Rep 2022;12:11372.ArticlePubMedPMCPDF
- 36. Kim Y. The Korea National Health and Nutrition Examination Survey (KNHANES): current status and challenges. Epidemiol Health 2014;36:e2014002.ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite