Articles
- Page Path
- HOME > Epidemiol Health > Volume 46; 2024 > Article
-
COVID-19
Original Article
Influence of practice location on prescribing, diabetes care, and colorectal cancer screening among Czech general practitioners during the COVID-19 pandemic -
Jan Bělobrádek1
 , Luděk Šídlo2, Tom Philipp3,4
, Luděk Šídlo2, Tom Philipp3,4 -
Epidemiol Health 2024;46:e2024033.
DOI: https://doi.org/10.4178/epih.e2024033
Published online: February 23, 2024
1Institute of Preventive Medicine, Charles University Faculty of Medicine in Hradec Králové, Hradec Králové, Czech Republic
2Department of Demography and Geodemography, Charles University Faculty of Science, Praha, Czech Republic
3General Health Insurance Company (GHIC), Praha, Czech Republic
4Charles University, Third Faculty of Medicine, Rheumatology and Rehabilitation Clinic, Praha, Czech Republic
- Correspondence: Jan Bělobrádek Institute of Preventive Medicine, Charles University Faculty of Medicine in Hradec Králové, Simkova 870, Hradec Kralove 500 03, Czech Republic E-mail: mudrjanbelobradek@gmail.com
© 2024, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,291 Views
- 80 Download
Abstract
-
OBJECTIVES
- The provision of primary health care was not interrupted during the coronavirus disease 2019 (COVID-19) pandemic in Czechia, although the capacity and resources of providers changed. We examined how the pandemic affected individual general practices throughout 2017-2021, focusing on differences between urban and rural practices.
-
METHODS
- We analysed data from the largest health insurance company in Czechia, which provides care to 4.5 million people (60% of the population). We evaluated the prescription volume, diabetes care procedures, and faecal immunochemical test (FIT) in preventive care and new pandemic-related procedures (remote consultations, testing, and vaccinations). For the spatial distribution of practices, we adapted the Organisation for Economic Cooperation and Development typology.
-
RESULTS
- We observed minimal declines in 2020 in the rate of prescribing (-1.0%) and diabetes care (-5.1%), with a rapid resumption in 2021, but a substantial decline in FIT (-17.8% in 2020) with slow resumption. Remote consultations were used by 94% of all practices regardless of location, with testing and vaccinations more commonly performed by rural general practitioners (GPs).
-
CONCLUSIONS
- Primary care in Czechia rose to the challenge of the COVID-19 pandemic, as shown by the finding that the volume of healthcare services provided through primary care did not decrease across most of the monitored parameters. This study also confirmed that rural GPs provide more care in-house, both in terms of prescribing and procedures performed in their practices. Future studies will need to focus on preventive care, which the pandemic has dampened in GP practices in Czechia.
- Primary care in Czechia has effectively adapted to the changes brought about by the COVID-19 pandemic. Minimal impact was observed in prescribtions and diabetic patient care. There was a significant decline in colorectal cancer screening, with a slow restitution after the pandemic subsided. Rural GPs consistently provided in-house treatment and have higher shares of both prescribing and diabetes care, as well as performing more COVID-19 specific procedures.
Key Message
- When coronavirus disease 2019 (COVID-19) was declared a pandemic in March 2020 [1], primary healthcare systems around the world had been undergoing unprecedented changes for several weeks [2,3] and were bracing for further transformations in the period ahead [4,5]. Prior recommendations were based solely on models of an influenza pandemic [6,7]. As a result, the full extent of the impact on the economy, social life, and healthcare systems during an actual pandemic like COVID-19 could not have been anticipated. Although primary care providers managed the initial surge of the disease on a global scale, several areas have been identified that will require future attention [8].
- The greatest concern remains the fate of patients who delayed their doctor visits during the pandemic for various reasons [9]. This group includes patients with chronic conditions who missed their regular follow-ups, potentially leading to inadequate management of their conditions and all associated negative outcomes, such as increased complications, hospitalisations, and mortality [10]. Additionally, the situation has led to a decline in preventive care, particularly evident in the reduced number of cancer screenings and diagnostic tests [11].
- The inappropriate geographic distribution of physicians, which disproportionately affects rural areas, has long been recognised as a global issue in primary care [12]. This challenge is not limited by the size or economic status of European countries [13,14]. Czechia has observed similar trends to those in neighbouring countries [15]. From 2010 to 2019, general practitioners (GPs) in Czechia have seen an increase in the average age of doctors, coupled with a territorially uneven and insufficient renewal of the workforce, with the slowest rates of replenishment occurring in rural regions [16]. These dynamics likely impacted the delivery of care during the COVID-19 pandemic, as the aging and understaffed network of rural GPs came under increased pressure from patients, particularly because they were often the sole healthcare coordinators available in their locations.
- While numerous papers have addressed the impact of the COVID-19 pandemic on primary care, emphasising the abrupt changes it necessitated—such as reduced patient contact, operational modifications due to anti-pandemic measures, testing and vaccinations, and the adoption of telemedicine [10,17]—our study sought to provide a more comprehensive perspective on the functioning of GP practices during this period. We focused on exploring how GPs adapted to the new responsibilities, including remote consultations, testing, and vaccinations, while also managing their customary pre-pandemic activities.
- The differences between rural and urban GP practices during the COVID-19 pandemic were demonstrated in the general conditions of providing care, as shown in an international comparison [18]. The breadth of the data we had access to enabled us to quantify these potential differences across various activities, improving our understanding of how GP practices functioned during the pandemic. Our goal was to determine whether the introduction of new activities—such as remote consultations, testing, and vaccinations—overwhelmed the capacity of GP practices, potentially displacing the activities that GPs typically performed before the pandemic. Since we had a robust dataset at our disposal, which might not provide sufficiently illustrative aggregate outputs, particularly in an international comparison, we opted to select procedures that we believe are sufficiently representative of individual GP activities. These procedures are also pertinent to primary care and can be easily understood in an international context.
- To evaluate the overall volume of healthcare services provided, we focused on the prescription patterns and their distribution between GPs and other doctors working in outpatient care. Despite international comparisons showing no reduction in the prescription of chronic disease medications during the COVID-19 pandemic [19], there was a notable decrease in antibiotic prescriptions [20]. We specifically monitored patients with diabetes receiving chronic care, as their management is a high health priority within the European Union (EU); diabetes accounted for 9% of EU healthcare costs in 2019 [21]. In the realm of preventive oncology care, we focused on the faecal immunochemical test (FIT), also known as the faecal occult blood test. The associated screening program aims to prevent colorectal carcinoma, which is another significant healthcare priority in the EU [22]. This concern is relevant to the entire population, unlike breast and cervical cancers.
- Concerning activities related to COVID-19, we assessed the frequency of remote consultations, the number of diagnostic tests administered (only antigen tests were conducted in GP practices in Czechia), and the administration of vaccinations. Given the phased implementation of these procedures, a comparison of individual pandemic years was not meaningful. In 2020, only a limited number of tests were carried out, and vaccinations commenced in centrally established vaccination centres. It was not until 2021 that the full capacity of GP practices was utilised for all the aforementioned activities.
- To categorise individual practices along the urban-rural spectrum, we employed a typology of general practices that we developed, drawing on the Organisation for Economic Cooperation and Development (OECD) typology, which has been consistently utilised in the authors’ prior research. To reduce errors in our assessment that could arise from overall changes in healthcare services, we selected a 5-year monitoring period (2017-2021). Within this timeframe, the initial 3 years were considered representative of typical conditions, while the latter 2 years were influenced by the COVID-19 pandemic.
INTRODUCTION
- Our data were obtained from the largest health insurance company in Czechia, the General Health Insurance Company of the Czech Republic (GHIC). During the period under review, the GHIC covered 5.9 million insured individuals, including 4.5 million adults, which represents approximately 60% of the Czech population [23]. Nearly all healthcare providers in Czechia have contracts with this health insurance company.
- We used anonymised data related to individual providers, identified by facility ID (as providers in Czechia may operate multiple practices), organised monthly for the years 2017-2021 [24]. Prescribing data was further divided into prescriptions written by GPs themselves and those written by other physicians in outpatient care, such as specialists and specialist hospital outpatient departments. For diabetes care, we evaluated the management of uncomplicated type 2 diabetes mellitus patients who were registered with practices by personal choice. It is important to note that GPs in Czechia do not manage type 1 diabetes mellitus or complicated type 2 diabetes mellitus patients—that is, those typically treated with incretins, sodium-glucose linked transporter 2 (SGLT2) inhibitors, thiazolidinediones, acarbose, glinides, and insulin—as their care is referred to specialists. Patient health checks adhere to the recommended frequency of 4 times per year. In terms of cancer screening, we analysed the outcomes of the “signal procedure–negative test” and the “signal procedure–positive test.” These procedures are automatically included in the contracts of all GP practices in Czechia, as the law mandates the performance of these screenings. Over the review period, there were changes in the testing methodology and the procedures reported. Consequently, the signal codes were the only reliable measure for evaluation.
- We assessed procedures directly linked to COVID-19 within the overall totals, taking no account of the fluctuations in legislative changes or the progressive development of the contractual framework with healthcare payers. Remote consultations emerged as a newly defined procedure, whereas testing primarily consisted of administering antigen tests (in Czechia, GPs were reimbursed solely for antigen tests, while specialised centres carried out polymerase chain reaction [PCR] tests). Regarding vaccinations, we tracked the total number of vaccine administrations, encompassing all vaccine types and including both initial vaccinations and booster doses.
- To categorise practices along the urban-rural spectrum, we employed a methodology previously described and utilised in other studies [16,25]. Following the OECD guidelines, we classified general practices into 3 categories: urban, intermediate, and rural. Another criterion for evaluation is the availability of a hospital offering acute care in at least 1 core specialty (internal medicine, surgery, paediatrics, or gynaecology) within the settlement. This categorisation is conducted at the level of municipalities with extended powers, which are smaller towns in Czechia that hold a regional level of competence in state administration. Consequently, the intermediate category was further divided into 2 subcategories: municipalities with extended powers that have such a hospital and those without. If a provider operates multiple practices across different categories, they were assigned to the category where they have the most contracted working hours. Table 1 displays the total number of practices for each year monitored, along with the proportion of each category.
MATERIALS AND METHODS
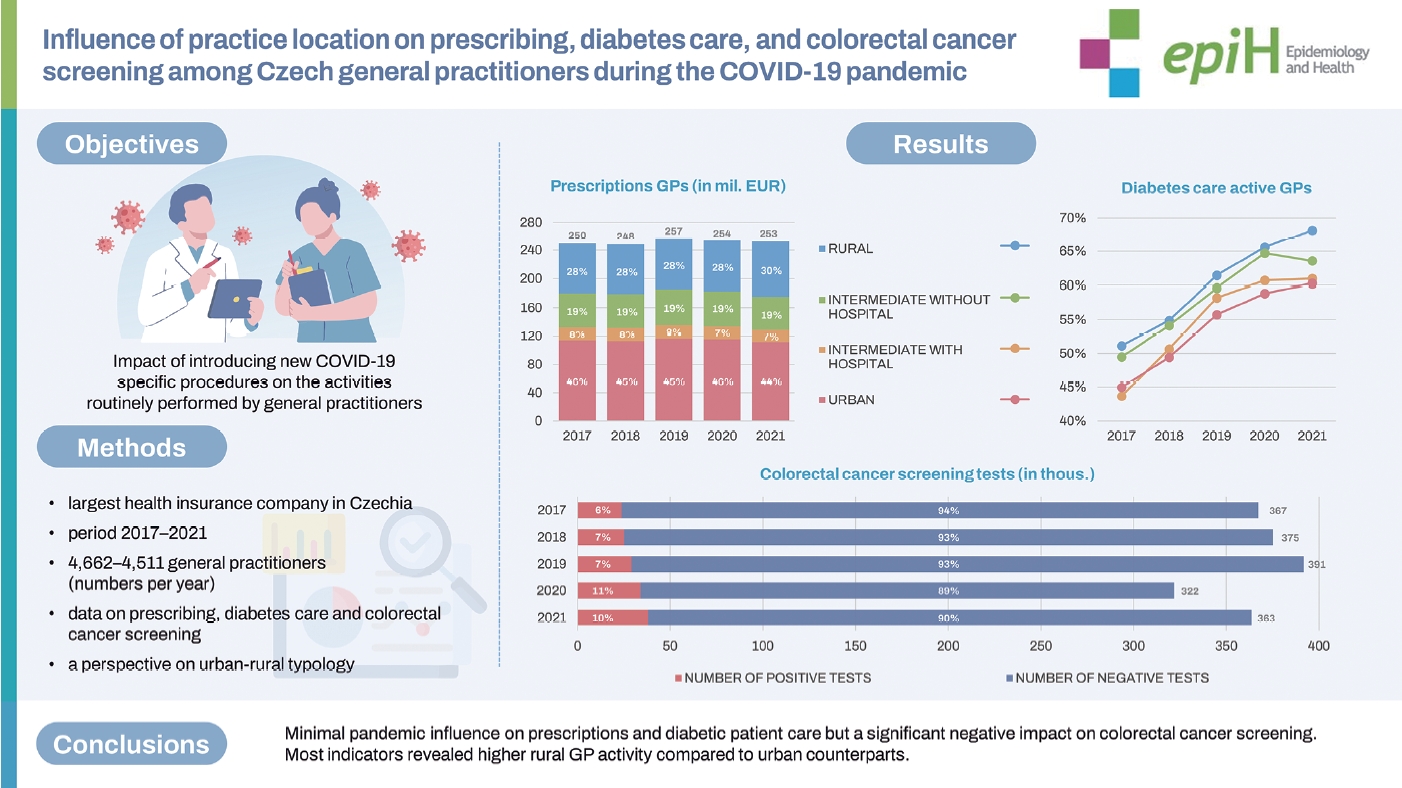
- Supplementary Material 1 presents the compiled data on prescription trends. The consistent annual increase in outpatient prescribing was disrupted in 2020 with a 1.0% decrease. However, in 2021, prescribing resumed its upward trajectory with a 3.2% increase. A comparison of different practice types revealed a slight decline in urban practices and a slight increase in rural practices. The distribution of these types aligned closely with the overall representation of general practices (Table 1). Specifically for GP prescribing, there was a notable shift in proportion favouring rural practices (Figure 1). This aligns with previous research indicating that rural general practices in Czechia tend to prescribe more medications in-house than their urban counterparts [28].
- Supplementary Material 2 presents data on GP care for patients with diabetes. Figure 2 illustrates a steady rise in the number of practices offering care for diabetes patients, a trend that persisted despite the COVID-19 pandemic. In 2020, there was a 5.1% reduction in the number of treatments; however, the volume of treatments rebounded to the 2019 levels by 2021. Although there was an increase in the proportion of GPs providing care for patients with diabetes towards the periphery, the distribution among different types of general practices remained relatively unchanged throughout the years under review and was seemingly unaffected by the COVID-19 pandemic.
- We observed different dynamics for colorectal cancer screening (Table 2). Prior to the COVID-19 pandemic, there was a slight increase in the total number of tests performed. However, there was a notable 17.8% decrease in 2020. This decline was solely due to a reduction in negative tests, which fell by 20.6% that year. Conversely, the number of positive tests actually increased, with a seemingly paradoxical peak in 2020, showing the highest year-on-year increase at 17.1%. In 2021, the volume of tests administered rebounded by 13%, yet the total remained comparable to the figures from 2017. Notably, the incidence of positive tests in 2021 was 60% higher than that observed in 2017.
- The specific procedures related to COVID-19 are provided in Table 3. They include remote consultations, tests, and vaccinations aggregated over the years 2020 and 2021. There was a notably high utilisation of remote consultations, with over 94% of GP practices employing this method. The distribution of these consultations did not vary by practice type when compared to the total number of practices. Regarding testing, rural practices conducted a greater number of tests than their urban counterparts (44.2 vs. 30.7%), despite representing only half as many practices. Similarly, rural practices were more prominently represented in vaccination efforts, a trend that was also supported by intermediate-type practices without hospitals, which displayed characteristics akin to those of rural practices. The overall participation of general practices in administering COVID-19 vaccinations was nearly 86%.
RESULTS
- We consider the data from the largest health insurer in Czechia to be sufficiently representative due to its robustness and nationwide coverage, despite the variation in the share of the insured across different regions. This variation could primarily affect quantitative indicators. However, because our comparison did not focus on individual regions but rather on types of practices within a relatively stable network over time, and because we conducted longitudinal monitoring of the same indicators across consecutive years, we do not view the uneven territorial density of the insured as a methodological barrier in this type of comparison.
- At the same time, we have chosen a subset of indicators from the data, which include the total costs of outpatient care for insured patients. This encompassed services provided by GPs and specialists, such as procedures, prescriptions, laboratory tests, diagnostic radiography, home care, capitation, and bonuses, amounting to approximately EUR 2.5 billion per year. These indicators are representative of the care provided. Assessing the total costs at the individual practice level is challenging due to their inherent disproportionality. The indicators we selected are specific to GPs and are uniformly utilised across all practices in Czechia. This is in contrast to certain instrumental procedures, such as electrocardiography (ECG) and point-of-care testing (POCT), which are adopted voluntarily by practices and are not uniformly distributed [26].
- Changes in the number of treatments during the COVID-19 pandemic, including economic indicators, have been studied in several European countries. These studies have consistently reported a decrease in in-person patient visits to medical practices, with a shift towards remote consultations. However, the time frames examined were often brief, such as the years 2019-2020 in Catalonia [27] and France [28]. In France, for example, there was a notably greater reduction in specialist activities compared to those of GPs [29]. A study conducted in Poland also had a narrow focus, highlighting the shortcomings of the capitation reimbursement system in adapting to pandemic conditions [30]. Our findings indicate a minimal decrease in total outpatient prescribing in 2020, suggesting that the care for chronic patients was not significantly compromised. We did not observe any substantial changes in the ratio of GP prescribing (consistently one-quarter) to other outpatient prescribing (consistently three-quarters) over the long term. The proportion of GP prescribing has been on a slight decline over an extended period. The COVID-19 pandemic appears to have had no impact on this long-standing trend.
- In Canada, there was a reported decrease in the number of visits by patients with diabetes and assessments for organ complications [31]. Similarly, the United Kingdom experienced a drop in the prescribing rates for individuals with diabetes [32]. The pandemic has also introduced several challenges in the long-term management of these patients. While the reduction in routine health checks at clinics may have protected patients with diabetes from the virus, it also heightened the risk of disrupted comprehensive care. This includes delays in consultations for complications, issues with medication availability and adherence, and decreased physical activity due to lockdowns [33]. A study from the United States examined the total number and types of visits, as well as diabetes care and cancer screenings, in 2020. The study observed a slow and partial recovery to pre-pandemic levels [34]. Our findings indicate a decrease in diabetes treatment in 2020, followed by a swift rebound to the levels seen in 2019. The pandemic did not curb the growing proportion of GP practices providing diabetes care, which is an encouraging development. Moreover, the increased involvement of rural practices in diabetes care aligns with previous research, which found that rural general practices in Czechia tend to offer more comprehensive services in-house compared to their urban counterparts [25].
- Concerns regarding the impact of reduced colorectal cancer screenings were highlighted at the onset of the pandemic [35,36]. This downturn was observed on a global scale [37,38]. However, there was also a report of a rapid resumption of screening examinations once restrictions were lifted [39]. Despite this, apprehensions about the disruption of screening programs remained widespread. Experts deliberated on which high-risk patient groups should continue to receive cancer screenings, even amidst a pandemic [40]. Our findings indeed indicate a decline in the total number of tests, but this was solely for negative results; the number of positive tests actually rose on a year-over-year basis during the COVID-19 pandemic. This could be attributed to 2 factors: (1) a shift in the testing method—throughout the period in question, physicians adopted the quantitative POCT with a fixed cutoff, leading to an uptick in positive results starting from 2019; and (2) a more selective approach by GPs during the pandemic. The restoration of testing numbers post-pandemic was considerably slower compared to diabetes care. By 2021, the figures nearly returned to those of 2017.
- The COVID-19 pandemic transformed theoretical assumptions about the potential of telemedicine in primary health care into a tangible reality. The initial recommendations for remote patient consultations were promptly introduced [17,41], and they quickly became the standard of care for a wide range of diagnoses, not solely for COVID-19 [42]. Physicians began to recognise the future benefits of telemedicine, while also voicing concerns about patients lacking access to the necessary technology [43]. Notably, primary care physicians had a more positive evaluation of telemedicine’s potential and utilised it more frequently than specialists did. This positive assessment and increased usage were particularly evident among female physicians [44]. In Czechia, remote contact was officially recognised as a medical procedure on September 1, 2020. However, its practical implementation was gradual. Some health insurance companies were slow to adopt it and later imposed restrictions, leading to uncertainties about reporting that discouraged some physicians from using it. Similar to trends in other countries, telephone consultations were much more common than video consultations [45]. Despite these challenges, telemedicine has become established and continues to be used today, albeit with some modifications and limitations on the frequency of use in the list of reimbursed procedures.
- The involvement of GPs in testing and vaccination efforts in Czechia was influenced by the overall availability of diagnostic tests and vaccines, as well as by changing legislation, which included repeated mandates for widespread testing. This was further complicated by the gradual implementation of relevant procedures by health insurance companies. Consequently, the role of GPs in these activities was heavily regulated, and the frequent changes in regulations and reimbursement policies led to a reluctance among many physicians to participate. Across the country, many accredited centres conducted PCR tests, while antigen testing was primarily allocated to primary healthcare settings, companies, schools, and the general public. In a similar vein, during the initial vaccine shortage, vaccination centres were the preferred venues for administering shots. It was only later that vaccinations became more commonly available in general practices. The close proximity of dedicated testing and vaccination centres negatively impacted GPs’ willingness to be involved in these activities.
- Primary care in Czechia effectively managed the tasks brought on by the COVID-19 pandemic, reflecting many trends observed internationally. It is noteworthy that, with the exception of cancer screening, there was no significant decline in the volume of activities that had been carried out for many years. The sector merely experienced a pause in the continuous growth that had been documented in the years preceding the pandemic. Furthermore, primary care was able to adapt to changes in the organisation of health care services, such as remote consultations, and to incorporate new responsibilities, including testing and vaccinations, brought about by the pandemic.
- Of the GP activities we monitored, there was a slight decrease in the treatment of patients with diabetes during the pandemic. However, the number of colorectal cancer screening tests conducted experienced a more pronounced decrease. Although the treatment of diabetes patients rebounded to 2019 levels by 2021, the recovery in colorectal cancer screening procedures was considerably slower. Notably, the number of positive results from colorectal screening tests continued to rise during the pandemic, which was an unexpected outcome. This trend may be partly attributed to the change in screening methodology that was implemented between 2018 and 2019.
- The total volume of prescriptions in outpatient care decreased by only 1% in 2020, indicating that the availability of medical care did not significantly deteriorate during the pandemic. The long-term trends in the proportion of prescriptions issued by GPs compared to other physicians, as well as the distribution of prescriptions between urban and rural GPs, were not significantly altered by the COVID-19 pandemic. Rural GPs consistently provided in-house treatment and have higher shares of both prescribing and diabetes care. Furthermore, we demonstrated their increased participation in COVID-19-related procedures, including both testing and vaccinations.
- The new procedure of remote consultation was adopted widely among GPs, with a utilisation rate of 94%. This practice has persisted even after adjustments to the conditions, and it continues to be covered by health insurance companies. Looking ahead, it will be essential to monitor how GP activities in Czechia are evolving in response to the COVID-19 pandemic, with particular attention to preventive care and cancer screening programs.
DISCUSSION
Supplementary materials
Supplementary Material 1.
-
Conflict of interest
The authors have no conflicts of interest to declare for this study.
-
Funding
None.
-
Author contributions
Conceptualization: Bělobrádek J, Šídlo L. Data curation: Bělobrádek J, Šídlo L, Philipp T. Formal analysis: Šídlo L. Funding acquisition: None. Methodology: Bělobrádek J, Šídlo L. Project administration: Philipp T. Visualization: Šídlo L. Writing – original draft: Bělobrádek J, Šídlo L, Philipp T. Writing – review & editing: Bělobrádek J, Šídlo L, Philipp T.
NOTES
ACKNOWLEDGEMENTS



| Variables | 2017 (n=4,662) | 2018 (n=4,630) | 2019 (n=4,595) | 2020 (n=4,560) | 2021 (n=4,511) | Population ≥15 (%)2 |
|---|---|---|---|---|---|---|
| Urban | 2,485 (53.3) | 2,469 (53.3) | 2,452 (53.4) | 2,436 (53.4) | 2,370 (52.5) | 43.9 |
| Intermediate with hospital | 293 (6.3) | 288 (6.2) | 285 (6.2) | 280 (6.1) | 269 (6.0) | 5.2 |
| Intermediate without hospital | 762 (16.3) | 761 (16.4) | 758 (16.5) | 754 (16.6) | 738 (16.4) | 12.6 |
| Rural | 1,122 (24.1) | 1,112 (24.1) | 1,100 (23.9) | 1,090 (23.9) | 1,134 (25.1) | 38.3 |
Values are presented as absolute numbers and, in brackets, relative numbers in %.
1 Modified from General Health Insurance Company of the Czech Republic; Unpublished dataset with anonymised data for reported healthcare for GP providers provided for analysis, 2022 [24].
2 Population ≥15=structure of the population aged 15 and over (GPs’ patients), 8.9 million in total (as of 1 July 2019, mid-term).
Values are presented as %.
GP, general practitioner; GHIC, General Health Insurance Company of the Czech Republic.
1 Modified from GHIC; Unpublished dataset with anonymised data for reported healthcare for GP providers provided for analysis, 2022 [24].
COVID-19, coronavirus disease 2019; GP, general practitioner; GHIC, General Health Insurance Company of the Czech Republic.
1 Modified from GHIC; Unpublished dataset with anonymised data for reported healthcare for GP providers provided for analysis, 2022 [24].
- 1. World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19-11 March 2020 [cited 2023 Jun 10]. Available from: https://www.who.int/directorgeneral/speeches/detail/who-director-general-s-opening-remarksat-the-media-briefing-on-covid-19---11-march-2020.
- 2. Rawaf S, Allen LN, Stigler FL, Kringos D, Quezada Yamamoto H, van Weel C, et al. Lessons on the COVID-19 pandemic, for and by primary care professionals worldwide. Eur J Gen Pract 2020;26:129-133 https://doi.org/10.1080/13814788.2020.1820479.ArticlePubMedPMC
- 3. Khalil-Khan A, Khan MA. The impact of COVID-19 on primary care: a scoping review. Cureus 2023;15:e33241. https://doi.org/10.7759/cureus.33241.ArticlePubMedPMC
- 4. Groenewegen P, Van Poel E, Spreeuwenberg P, Batenburg R, Mallen C, Murauskiene L, et al. Has the COVID-19 pandemic led to changes in the tasks of the primary care workforce? An international survey among general practices in 38 countries (PRICOV-19). Int J Environ Res Public Health 2022;19:15329 https://doi.org/10.3390/ijerph192215329.ArticlePubMedPMC
- 5. Windak A, Frese T, Hummers E, Klemenc Ketis Z, Tsukagoshi S, Vilaseca J, et al. Academic general practice/family medicine in times of COVID-19 - perspective of WONCA Europe. Eur J Gen Pract 2020;26:182-188 https://doi.org/10.1080/13814788.2020.1855136.ArticlePubMedPMC
- 6. Holloway R, Rasmussen SA, Zaza S, Cox NJ, Jernigan DB. Updated preparedness and response framework for influenza pandemics. MMWR Recomm Rep 2014;63:1-18.
- 7. Qualls N, Levitt A, Kanade N, Wright-Jegede N, Dopson S, Biggerstaff M, et al. Community mitigation guidelines to prevent pandemic influenza - United States, 2017. MMWR Recomm Rep 2017;66:1-34 https://doi.org/10.15585/mmwr.rr6601a1.ArticlePubMedPMC
- 8. Organisation for Economic Cooperation and Development (OECD). Strengthening the frontline: how primary health care helps health systems adapt during the COVID 19 pandemic. Paris: OECD Publishing; 2021 https://doi.org/10.1787/9a5ae6da-en.
- 9. Feral-Pierssens AL, Claret PG, Chouihed T. Collateral damage of the COVID-19 outbreak: expression of concern. Eur J Emerg Med 2020;27:233-234 https://doi.org/10.1097/MEJ.0000000000000717.ArticlePubMedPMC
- 10. Van Poel E, Vanden Bussche P, Klemenc-Ketis Z, Willems S. How did general practices organize care during the COVID-19 pandemic: the protocol of the cross-sectional PRICOV-19 study in 38 countries. BMC Prim Care 2022;23:11 https://doi.org/10.1186/s12875-021-01587-6.ArticlePubMedPMC
- 11. Jones D, Neal RD, Duffy SR, Scott SE, Whitaker KL, Brain K. Impact of the COVID-19 pandemic on the symptomatic diagnosis of cancer: the view from primary care. Lancet Oncol 2020;21:748-750 https://doi.org/10.1016/S1470-2045(20)30242-4.ArticlePubMedPMC
- 12. Ono T, Schoenstein M, Buchan J. Geographic imbalances in doctor supply and policy responses. OECD Health Working Papers, No. 69. Paris: OECD Publishing; 2014 https://doi.org/10.1787/5jz5sq5ls1wl-en.
- 13. World Heatlh Organization. Imbalances in rural primary care: a scoping literature review with an emphasis on the WHO European; 2020 [cited 2023 Jun 10]. Available form: https://apps.who.int/iris/bitstream/handle/10665/346351/WHO-HIS-SDS-2018.58-eng.pdf?sequence= 1.
- 14. Groenewegen PP, Bosmans MW, Boerma WG, Spreeuwenberg P. The primary care workforce in Europe: a cross-sectional international comparison of rural and urban areas and changes between 1993 and 2011. Eur J Public Health 2020;30(Suppl_4):iv12-iv17 https://doi.org/10.1093/eurpub/ckaa125.ArticlePubMedPMC
- 15. Sídlo L. Demographic view on primary health care physicians in the Czech Republic--present state as headstone for the future development. Cas Lek Cesk 2010;149:563-571 (Czech).PubMed
- 16. Šídlo L, Bělobrádek J, Maláková K. General medical practitioners in Czechia: development trends and regional differences. Geografie 2021;126:169-194 (Czech). https://doi.org/10.37040/geografie2021126020169.Article
- 17. Greenhalgh T, Koh GC, Car J. Covid-19: a remote assessment in primary care. BMJ 2020;368:m1182 https://doi.org/10.1136/bmj.m1182.ArticlePubMed
- 18. Petrazzuoli F, Collins C, Van Poel E, Tatsioni A, Streit S, Bojaj G, et al. Differences between rural and urban practices in the response to the COVID-19 pandemic: outcomes from the PRICOV-19 study in 38 countries. Int J Environ Res Public Health 2023;20:3674 https://doi.org/10.3390/ijerph20043674.ArticlePubMedPMC
- 19. Selke Krulichová I, Selke GW, Bennie M, Hajiebrahimi M, Nyberg F, Fürst J, et al. Comparison of drug prescribing before and during the COVID-19 pandemic: a cross-national European study. Pharmacoepidemiol Drug Saf 2022;31:1046-1055 https://doi.org/10.1002/pds.5509.ArticlePubMedPMC
- 20. Högberg LD, Vlahović-Palčevski V, Pereira C, Weist K, Monnet DL; ESAC-Net study group, et al. Decrease in community antibiotic consumption during the COVID-19 pandemic, EU/EEA, 2020. Euro Surveill 2021;26:2101020 https://doi.org/10.2807/1560-7917.ES.2021.26.46.2101020.ArticlePubMedPMC
- 21. European Parliament. European Parliament resolution of 23 November 2022 on prevention, management and better care of diabetes in the EU on the occasion of World Diabetes Day [cited 2023 Jun 10]. Available from: https://www.europarl.europa.eu/doceo/document/TA-9-2022-0409_EN.html.
- 22. European Commission. Cancer screening, diagnosis and care [cited 2023 Jun 10]. Available from: https://healthcare-quality.jrc.ec.europa.eu/en.
- 23. General Health Insurance Company of the Czech Republic. 2022 Yearbooks [cited 2023 Jun 10]. Available form: https://www.vzp.cz/o-nas/dokumenty/rocenky (Czech).
- 24. General Health Insurance Company of the Czech Republic. Unpublished dataset with anonymised data for reported healthcare for general practitioner providers provided for analysis. Praha: General Health Insurance Company of the Czech Republic; 2022. (Czech).
- 25. Bělobrádek J, Šídlo L, Javorská K, Halata D. Urban or rural GP? In the Czech Republic it is not just distances that matter. Acta Medica (Hradec Kralove) 2021;64:15-21 https://doi.org/10.14712/18059694.2021.3.ArticlePubMed
- 26. Bělobrádek J, Šídlo L, Maláková K. Using selected POCT methods by general practitioners in the Czech Republic. Cas Lek Cesk 2021;160:185-192.PubMed
- 27. Lopez Segui F, Hernandez Guillamet G, Pifarré Arolas H, MarinGomez FX, Ruiz Comellas A, Ramirez Morros AM, et al. Characterization and identification of variations in types of primary care visits before and during the COVID-19 pandemic in Catalonia: big data analysis study. J Med Internet Res 2021;23:e29622. https://doi.org/10.2196/29622.ArticlePubMedPMC
- 28. Tuppin P, Lesuffleur T, Constantinou P, Atramont A, Coatsaliou C, Ferrat E, et al. Underuse of primary healthcare in France during the COVID-19 epidemic in 2020 according to individual characteristics: a national observational study. BMC Prim Care 2022;23:200 https://doi.org/10.1186/s12875-022-01792-x.ArticlePubMedPMC
- 29. Davin-Casalena B, Jardin M, Guerrera H, Mabille J, Tréhard H, Lapalus D, et al. The impact of the COVID-19 epidemic on primary care in South-eastern France: implementation of a real-time monitoring system based on regional health insurance system data. Rev Epidemiol Sante Publique 2021;69:255-264 (French). https://doi.org/10.1016/j.respe.2021.07.006.ArticlePubMedPMC
- 30. Korneta P, Kludacz-Alessandri M, Walczak R. The impact of COVID-19 on the performance of primary health care service providers in a capitation payment system: a case study from Poland. Int J Environ Res Public Health 2021;18:1407 https://doi.org/10.3390/ijerph18041407.ArticlePubMedPMC
- 31. Moin JS, Troke N, Plumptre L, Anderson GM. Impact of the COVID-19 pandemic on diabetes care for adults with type 2 diabetes in Ontario, Canada. Can J Diabetes 2022;46:715-721 https://doi.org/10.1016/j.jcjd.2022.04.009.ArticlePubMedPMC
- 32. Carr MJ, Wright AK, Leelarathna L, Thabit H, Milne N, Kanumilli N, et al. Impact of COVID-19 restrictions on diabetes health checks and prescribing for people with type 2 diabetes: a UK-wide cohort study involving 618 161 people in primary care. BMJ Qual Saf 2022;31:503-514 https://doi.org/10.1136/bmjqs-2021-013613.ArticlePubMedPMC
- 33. Beran D, Aebischer Perone S, Castellsague Perolini M, Chappuis F, Chopard P, Haller DM, et al. Beyond the virus: ensuring continuity of care for people with diabetes during COVID-19. Prim Care Diabetes 2021;15:16-17 https://doi.org/10.1016/j.pcd.2020.05.014.ArticlePubMedPMC
- 34. Kim E, Kojima N, Vangala S, Dermenchyan A, Lambrechts S, Grossman M, et al. Impact of COVID-19 on primary care quality measures in an academic integrated health system. J Gen Intern Med 2022;37:1161-1168 https://doi.org/10.1007/s11606-021-07193-7.ArticlePubMedPMC
- 35. Del Vecchio Blanco G, Calabrese E, Biancone L, Monteleone G, Paoluzi OA. The impact of COVID-19 pandemic in the colorectal cancer prevention. Int J Colorectal Dis 2020;35:1951-1954 https://doi.org/10.1007/s00384-020-03635-6.ArticlePubMedPMC
- 36. Loveday C, Sud A, Jones ME, Broggio J, Scott S, Gronthound F, et al. Prioritisation by FIT to mitigate the impact of delays in the 2-week wait colorectal cancer referral pathway during the COVID-19 pandemic: a UK modelling study. Gut 2021;70:1053-1060 https://doi.org/10.1136/gutjnl-2020-321650.ArticlePubMedPMC
- 37. Mazidimoradi A, Tiznobaik A, Salehiniya H. Impact of the COVID-19 pandemic on colorectal cancer screening: a systematic review. J Gastrointest Cancer 2022;53:730-744 https://doi.org/10.1007/s12029-021-00679-x.ArticlePubMedPMC
- 38. Patel S, Issaka RB, Chen E, Somsouk M. Colorectal cancer screening and COVID-19. Am J Gastroenterol 2021;116:433-434 https://doi.org/10.14309/ajg.0000000000000970.ArticlePubMedPMC
- 39. Lee JK, Lam AY, Jensen CD, Marks AR, Badalov J, Layefsky E, et al. Impact of the COVID-19 pandemic on fecal immunochemical testing, colonoscopy services, and colorectal neoplasia detection in a large United States community-based population. Gastroenterology 2022;163:723-731.e6 https://doi.org/10.1053/j.gastro.2022.05.014.ArticlePubMedPMC
- 40. Fagundes TP, Albuquerque RM, Miranda DL, Landeiro LC, Ayres GS, Correia CC, et al. Dealing with cancer screening in the COVID-19 era. Rev Assoc Med Bras (1992) 2021;67(Suppl 1):86-90 https://doi.org/10.1590/1806-9282.67.suppl1.20200889.Article
- 41. Petrazzuoli F, Kurpas D, Vinker S, Sarkisova V, Eleftheriou A, Żakowicz A, et al. COVID-19 pandemic and the great impulse to telemedicine: the basis of the WONCA Europe Statement on Telemedicine at the WHO Europe 70th Regional Meeting September 2020. Prim Health Care Res Dev 2021;22:e80. https://doi.org/10.1017/S1463423621000633.ArticlePubMedPMC
- 42. Mohammed HT, Hyseni L, Bui V, Gerritsen B, Fuller K, Sung J, et al. Exploring the use and challenges of implementing virtual visits during COVID-19 in primary care and lessons for sustained use. PLoS One 2021;16:e0253665. https://doi.org/10.1371/journal.pone.0253665.ArticlePubMedPMC
- 43. Gomez T, Anaya YB, Shih KJ, Tarn DM. A qualitative study of primary care physicians’ experiences with telemedicine during COVID-19. J Am Board Fam Med 2021;34(Suppl):S61-S70 https://doi.org/10.3122/jabfm.2021.S1.200517.ArticlePubMed
- 44. Knörr V, Dini L, Gunkel S, Hoffmann J, Mause L, Ohnhäuser T, et al. Use of telemedicine in the outpatient sector during the COVID-19 pandemic: a cross-sectional survey of German physicians. BMC Prim Care 2022;23:92 https://doi.org/10.1186/s12875-022-01699-7.ArticlePubMedPMC
- 45. Petrazzuoli F, Gokdemir O, Antonopoulou M, Blahova B, MrduljašĐujić N, Dumitra G, et al. Patient consultations during SARSCoV-2 pandemic: a mixed-method cross-sectional study in 16 European countries. Rural Remote Health 2022;22:7196 https://doi.org/10.22605/RRH7196.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite