
Articles
- Page Path
- HOME > Epidemiol Health > Volume 46; 2024 > Article
-
Original Article
Associations of active and passive tobacco exposure with elevated blood pressure in Korean adolescents -
Hyerin Park1
 , Hyunsuk Jeong2, Hyeon Woo Yim2, Sanghyuk Bae2
, Hyunsuk Jeong2, Hyeon Woo Yim2, Sanghyuk Bae2 -
Epidemiol Health 2024;46:e2024028.
DOI: https://doi.org/10.4178/epih.e2024028
Published online: February 13, 2024
1Graduate School of Public Health and Healthcare Management, The Catholic University of Korea, Seoul, Korea
2Department of Preventive Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
- Correspondence: Hyunsuk Jeong Department of Preventive Medicine, College of Medicine, The Catholic University of Korea, 222 Banpo-dero, Seocho-gu, Seoul 06591, Korea E-mail: suejeong@catholic.ac.kr
© 2024, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,159 Views
- 182 Download
Abstract
-
OBJECTIVES
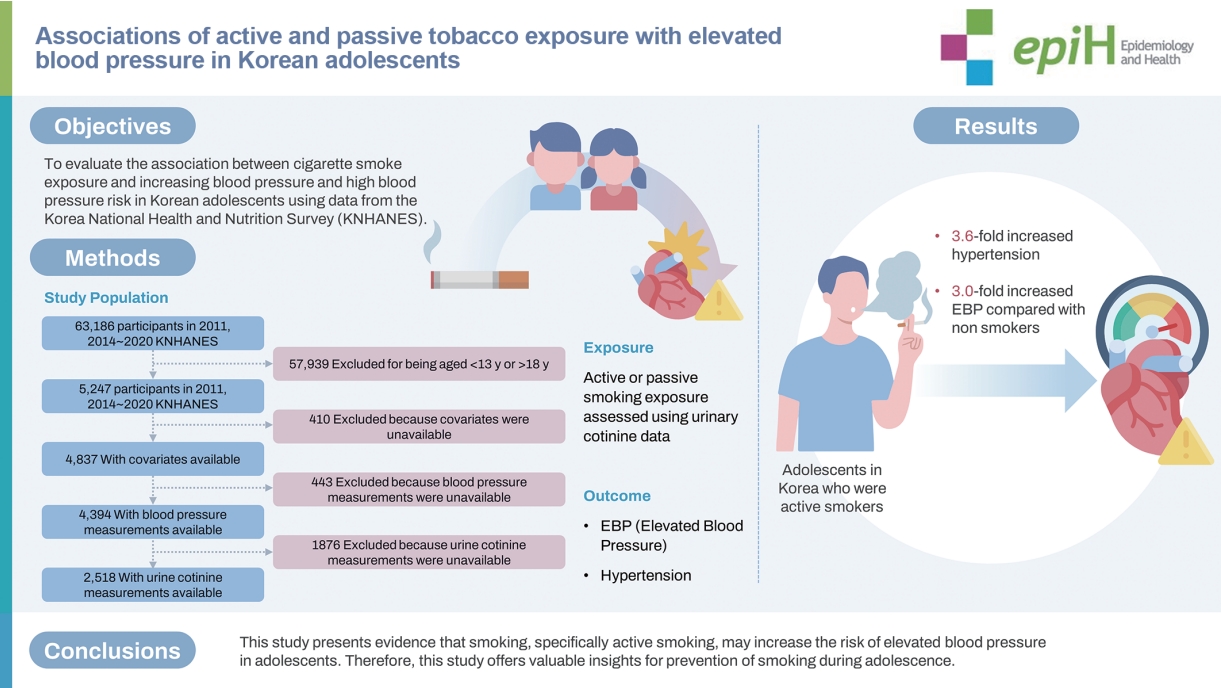
- To test the hypothesis that tobacco exposure is associated with elevated blood pressure (EBP) in Korean adolescents, and that the association is dose dependent.
-
METHODS
- This cross-sectional study used data from the 2011-2020 Korea National Health and Nutrition Survey (KNHANES). Subjects were eligible if they were 13-18 years at the time of participation in KNHANES. Tobacco exposure was defined by urine cotinine level. The main outcomes were EBP and hypertension. Statistical analyses were conducted using SAS version 9.4 with appropriate sampling weights to account for the complex survey design, stratification, and cluster variable.
-
RESULTS
- A total of 2,518 adolescents was included in the analysis, representing 2.5 million Korean adolescents. The mean± standard deviation participant age was 15.3±1.7 years, and 55.3% were male. The number of participants with active tobacco smoke exposure was 283 (11.2%), passive tobacco smoke exposure was 145 (5.8%), and no smoke exposure was 2,090 (83.0%). Analysis of the 2,518 urine-cotinine-verified participants showed that tobacco smoke exposure had a significant effect on EBP: with an odds of elevated blood pressure of 3.00 (95% confidence interval [CI], 1.14 to 7.89). The odds of hypertension were 3.61 (95% CI, 1.13 to 11.49) in the active smoking group compared with the no tobacco exposure group after adjustment for potential confounders.
-
CONCLUSIONS
- It is necessary to present a range of public health plans to reduce tobacco exposure that affects adolescents’ blood pressure, and further research with a larger number of participants using urine cotinine as a biomarker is needed.
- Hypertension during adolescence is a leading cause of disease in adults. The relationship between smoking and hypertension has been studied, but findings between studies are conflicting. Nicotine is a known toxin, but the relationship between active and passive smoking and blood pressure in adolescents is not clear. So that we tested and found adolescents in Korea who were active smokers showed over 3-fold increased risk of elevated blood pressure.
Key Message
- Hypertension is a chronic disease that highly impacts health and health care costs [1]. Awareness, treatment, and control of hypertension have been increasing due to multidisciplinary public health programs and policies, but disease prevalence has not decreased [2]. Hypertension in adults is affiliated with numerous and serious sequelae, including stroke and cardiovascular and kidney diseases. Although hypertension in adolescents is not directly related to cardiovascular disease and mortality, many studies have shown that hypertension in children and adolescents is associated with adult hypertension [3].
- Prevalence of hypertension in children and adolescents is around 1-5%, of which about 80% is the result of secondary conditions such as family history, body mass index (BMI), nutrition, and socioeconomic status [4]. Several studies have shown that smoking is a risk factor for hypertension, and exposure to cigarette smoking has an adverse effect on health throughout the lifespan [5,6]. One study reported that smoking was not significantly related to hypertension in children and adolescents [4]. In contrast, a recent study of data from the U.S.’ National Health and Nutrition Examination Survey (NHANES) reported that tobacco exposure in children and adolescents was significantly related to increased blood pressure [7].
- A cohort study of adults in Korea that reported that smoking, confirmed as urinary cotinine level, was associated with lower prevalence of hypertension in men but was not related to hypertension in the entire population or in women [8,9]. However, no study has evaluated the relationship between cigarette-smoke exposure and blood pressure. This study evaluated the association between cigarette smoke exposure and increasing blood pressure and high blood pressure risk in Korean adolescents using data from the Korea National Health and Nutrition Survey (KNHANES).
INTRODUCTION
- Study population
- In this secondary-analysis study, we used data on KNHANES from 2011-2020 excluding years 2012 and 2013 as urinary cotinine was not measured. All survey protocols were approved by the Korea Disease Control and Prevention Agency (KDCA). Participants were included if they were 13-18 years old and had available blood pressure and urinary cotinine data. Of the 63,186 participants in the 2011-2020 KNHANES, 5,247 met the age criterion, but 410 were missing covariate data, 443 did not have blood pressure measurements, and 1,876 did not have urine cotinine measurements (Figure 1). Ultimately, 2,518 participants were included in the analyses.
- Main exposure variable
- Tobacco exposure was divided into active and passive categories. Active smoking was defined as a urine cotinine level greater than or equal to 100 ng/mL, and passive smoking was defined as a urine cotinine level greater than or equal to 5 ng/mL and less than 100 ng/mL [10].
- Urine cotinine level was measured by gas chromatography mass spectrometry using a Perkin Elmer Clarus 600T (Perkin Elmer, Turku, Finland) and high-performance liquid chromatography mass spectrometry using the Agilent 1100 Series with the API 4000 (AB Sciex, Redwood City, CA, USA). The lower limit of detection of this assay is 0.5 ng/mL [11].
- Main outcome variables
- Elevated blood pressure (EBP) and hypertension were the main outcomes. All blood pressure measurements were performed manually by four nurses. Blood pressure was measured three times, and the average of the second and third measurements was used as the final value. EBP was defined as systolic/diastolic blood pressure greater than 120/80 mmHg, and hypertension was defined as systolic/diastolic blood pressure greater than 130/80 mmHg.
- Covariates
- Variables that directly or indirectly affect smoking and blood pressure were identified from a literature review, and we used directed acyclic graph (DAG) analysis to identify minimal sufficient adjustment sets of confounders [12]. Age, sex, BMI, family smoking status, stress, and household income were included as confounding variables. The DAG results are presented in Supplementary Material 1. BMI was categorized into three groups-normal weight, overweight and obese-using the Pediatric and Adolescent Growth Chart 2017 [13]. Self-reported family smoking status was grouped as none, smoking, and not answered. Stress was divided into three categories–high (a report of very much or much), medium (a report of little or hardly), and not answered. Household income was classified into quartiles of low, medium low, medium high, and high. Among the confounding variables, the presence of missing values exceeding 70% for physical activity, and alcohol consumption was excluded from the analysis. Missing values for father’s and mother’s education were categorized into a single category and included in the analysis.
- Statistical analysis
- The differences in prevalence of EBP and hypertension were analyzed for adolescents with available urinary cotinine data. The socio-demographic characteristics of the study participants according to active and passive smoking exposure were presented as number (% weighted), and the statistical differences between the two groups were assessed using the Rao-Scott chi-square test. Additional socio-demographic characteristics of the study participants for the normal, EBP and hypertension group were presented in a comparable manner. The associations between EBP, hypertension prevalence, and active or passive smoking exposure were examined using PROC SURVEYLOGISTIC to estimate odds ratios (ORs) and 95% confidence intervals (CIs). All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), taking into account complex sampling design by including weights, stratification variables, and clustering variables. A p-value < 0.05 was considered statistically significant.
- Ethics statement
- This study received exemption approval from Catholic University Songeui Institutional Review Board (No. MC23EASI0023).
MATERIALS AND METHODS
- Participant characteristics
- A total of 2,518 adolescents aged 13-18 years was included in the analysis, representing 2.5 million Korean adolescents. Among them, 2,090 (83.0%) were non-smokers, 283 (11.2%) were active smokers, and 145 (5.8%) were passive smokers. Mean± standard deviation (SD) participant age was 15.3 ± 1.7 years, and 1,398 (55.3%) were males. The prevalence of EBP and hypertension for non-smokers was 4.8% and 3.1%, respectively; those for passive smokers were 4.1% and 3.3% and those for active smokers were 7.5% and 2.7% (Table 1). Active smokers were more likely than passive smokers to be older (mean± SD age, 16.7± 1.3 vs. 15.7±1.6 years), male (76.8 vs. 58.8%), have higher levels of stress (38.1 vs. 24.8%), and have no insurance (3.2 vs. 0.2%) or medical assistance (8.7 vs. 3.4%). The prevalence of family smoking was similar in the passive smoking group compared with the active smoking group (29.1 vs. 28.8%) (Table 1).
- When the total group of adolescents was divided by blood pressure levels, 2,301 (91.4%) were normal, 133 (5.3%) had EBP and 84 (3.3%) had hypertension. Differences were found in all sociodemographic characteristics excluding urine cotinine and residential type between the different blood pressure levels (Table 2).
- Associations between tobacco exposure and abnormal blood pressure
- The OR for EBP was 1.93 (95% CI, 0.86 to 4.32), and the OR for hypertension was 2.35 (95% CI, 0.88 to 6.27) for participants with tobacco exposure compared with no tobacco exposure after adjusting potential confounders, including age and sex. The exposure category (passive tobacco exposure vs. active smoking) showed association with EBP (OR, 3.00; 95% CI, 1.14 to 7.89) and hypertension (OR, 3.61; 95% CI, 1.13 to 11.49) in the active smoking group. The relationships with EBP (OR, 0.90; 95% CI, 0.29 to 2.85) and hypertension (OR, 1.11; 95% CI, 0.28 to 4.44) were not significant in the passive smoking group after adjusting for all confounding variables (Table 3). In addition to adjusting for age, we also controlled for survey year. This adjustment was made because individuals of the same age but born in different years may introduce a potential source of error in the results, as presented in Supplementary Material 2. The OR for EBP and hypertension in the male only group exhibited the same pattern as the total group but was not statistically significant (Supplementary Material 3).
- The association between a 1-ng/mL increase in urine cotinine and hypertension is shown in Table 4. The results show that a 1-ng/mL increase in urine cotinine tended to associate an increase in hypertension risk for both active and passive smokers, though the impact was not statistically significant.
- Sensitivity analysis was done with lower cut-off level of the urine cotinine for active smoking from the current 100 ng/mL to 50 ng/mL, as recommended by the Society for Research on Nicotine and Tobacco [14]. Following a sensitivity analysis, the active smoking group demonstrated congruent outcomes that OR 2.39 for EBP and 3.38 for the hypertension after adjusting potential confounders. The sensitivity analysis is presented as Supplementary Material 4.
RESULTS
- This study revealed that adolescents in Korea who were active smokers showed a 3.6-fold increased hypertension and a 3.0-fold increased risk of EBP compared with non-smokers. A recent study involving 8,520 participants from the U.S. NHANES reported a significant association between EBP and hypertension and active and passive exposure to tobacco smoke in children and adolescents, where the exposed group had a 1.31-times higher likelihood of disease compared with the non-exposed group [7]. Previous studies have also shown that tobacco smoke exposure has an impact on EBP in certain children [15,16]. Long-term smoking has been linked to development of arterial sclerosis in adults, and a significant and rapid increase in arterial stiffness immediately after smoking a single cigarette has been observed [17]. Studies have also reported that children exposed to tobacco smoke experience a deterioration in endothelial function relative to nonexposed children [18]. Based on animal experiments and clinical trials, it is widely recognized that smoking exerts its effects by primarily stimulating the sympathetic nervous system, including at the neuronal terminals. This mechanism is known to cause persistent increases in blood pressure and can lead to sudden arrhythmias [19].
- In a study analyzing data from Korea Youth Risk Behavior Web-based Survey (KYRBWS) conducted between 2005 and 2013, active smoking rates were reported as 14.4% for males and 4.6% for females, while passive smoking rates were 29.5% for males and 32.0% for females [20]. In the present study analyzing data from 2011 to 2020 from KNHANES, active smoking rates increased to 19.4% for males and 7.3% for females, while passive smoking rates decreased to 6.9% for males and 6.0% for females. It is important to note that the KYRBWS relies on self-reported surveys to determine smoking status. Therefore, the reported rates of active smoking may be underestimated compared to the actual prevalence. Additionally, the decrease in passive smoking rates may be influenced by the nationwide implementation of smoking bans in facilities such as restaurants and PC rooms, starting from 2013 under the amendment of the National Health Promotion Act by the Ministry of Health and Welfare.
- During smoking, nicotine is absorbed into the bloodstream through the lungs and rapidly reaches the brain. Approximately 70-80% of inhaled nicotine is converted to cotinine in the body, and 10-15% of cotinine is excreted in the urine, while the remainder is converted to 4-oxo-4 (3-pyridyl) butanoic acid (keto acid). About 85% of keto acid is further converted to 4-hydroxy-4-(3-pyridyl) butanoic acid (hydroxy acid) and excreted in the urine [21]. Cotinine is the primary metabolite of nicotine and is considered a reliable biomarker for assessing smoking exposure. Nicotine can increase blood pressure through various biological mechanisms, including mimicking the actions of the sympathetic nervous system, regulating the renin-angiotensin system, and upregulating arginine, vasopressin, and endothelin-1 [22-24].
- The association between tobacco exposure and EBP in children and adolescents has significant implications for public health. Notably, New Zealand has taken proactive measures to address smoking-related issues. In December 2022, legislation was passed, set to take effect in 2023, prohibiting the purchase of tobacco products by people born after January 1, 2009, throughout their lifetime. The objective of this legislation is to bring about a transformation in the smoking environment by restricting access to tobacco and reducing the number of tobacco retailers. These efforts aim to create an environment that discourages smoking and promotes better health outcomes among the population [25]. According to a press release from the KDCA in 2022, smoking-related deaths in 2019 in Korea numbered more than 58,000 people. Additionally, the estimated socioeconomic cost resulting from smoking was calculated as more than 12 trillion Korean won [26]. Furthermore, in 2019, Korea ranked fifth among the 36 Organization for Economic Cooperation and Development member countries for daily smoking rates among males aged 15 years and older [27]. Blood pressure during adolescence is associated with adult blood pressure, and EBP in adulthood is a recognized risk factor for cardiovascular diseases. Consequently, the impact of tobacco smoke exposure on elevation of blood pressure during adolescence is a significant focus in public health campaigns. Understanding and addressing this issue can contribute to preventive efforts aimed at reducing the burden of cardiovascular diseases in the population [7].
- Potential limitations of this study are that, according to domestic research, cotinine may not be detectable within three days of smoking cessation [28]. People who have abstained from smoking for more than a week may be classified as non-smokers, despite having a history of active smoking. This study adopted the categorization of cotinine levels based on existing literature, defining active smoking as >100 ng/mL, passive smoking as 5-100 ng/mL, and non-smoking as < 5 ng/mL [10]. However, other studies have utilized a different threshold, defining active smoking as ≥ 50 ng/mL [29]. This variation in classification thresholds introduces the potential for misclassification errors, and there is a possibility of including a significant number of passive smokers among the self-reported active smokers. Last, this is a cross-sectional that cannot determine causal relationships.
- However, this study utilized data from the nationally representative KNHANES, enabling a large-scale examination of the relationship between tobacco smoke exposure and blood pressure in adolescents. This study presents evidence that smoking, specifically active smoking, may increase the risk of EBP in adolescents. Therefore, this study offers valuable insights for prevention of smoking during adolescence. In future studies, it would be beneficial to conduct additional research targeting a larger number of adolescents using urine cotinine. This would provide more comprehensive insights into the relationship between tobacco smoke exposure and blood pressure among adolescents.
DISCUSSION
Data availability
Supplementary materials
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
Supplementary Material 4.
-
Conflict of interest
The authors have no conflicts of interest to declare for this study. Hyunsuk Jeong has been the deputy editor of the Epidemiology and Health since 2024. She was not involved in the review process.
-
Funding
None.
-
Author contributions
Conceptualization: Park H, Jeong H. Data curation: Park H, Jeong H. Formal analysis: Park H, Jeong H. Funding acquisition: None. Methodology: Park H, Jeong H, Yim HW, Bae S. Project administration: Park H, Jeong H. Visualization: Park H, Jeong H. Writing – original draft: Park H. Writing – review & editing: Park H, Jeong H, Yim HW, Bae S.
NOTES
ACKNOWLEDGEMENTS

| Characteristics | All (n=2,518) |
Tobacco smoke exposure |
p-value | ||
|---|---|---|---|---|---|
| None (n=2,090) | Passive (n=145) | Active (n=283) | |||
| Age (yr) | 15.3±1.7 | 15.1±1.7 | 15.7±1.6 | 16.7±1.3 | <0.001 |
| Sex | |||||
| Male | 1,398 (55.3) | 1,092 (51.2) | 87 (58.8) | 219 (76.8) | <0.0011 |
| Female | 1,120 (44.7) | 998 (48.8) | 58 (41.2) | 64 (23.2) | |
| Body mass index (kg/m2) | 21.6±3.9 | 21.5±3.9 | 21.7±3.8 | 21.9±3.9 | <0.001 |
| Normal | 1,957 (78.2) | 1,621 (78.7) | 106 (71.6) | 230 (78.7) | <0.0011 |
| Overweight | 239 (8.5) | 205 (8.9) | 17 (13.0) | 17 (8.9) | |
| Obese | 322 (13.3) | 264 (12.4) | 22 (15.4) | 36 (12.4) | |
| Family smoking | |||||
| None | 1,465 (56.3) | 1,272 (59.8) | 68 (41.7) | 125 (43.1) | <0.0011 |
| Smoking | 518 (21.5) | 395 (19.6) | 39 (29.1) | 84 (28.8) | |
| Not answered | 535 (22.2) | 423 (20.6) | 38 (29.2) | 74 (28.1) | |
| Stress | |||||
| High | 704 (28.5) | 565 (27.1) | 35 (24.8) | 104 (38.1) | <0.0012 |
| Medium | 1,802 (71.0) | 1,517 (72.5) | 109 (74.8) | 176 (60.8) | |
| Not answered | 12 (0.5) | 8 (0.4) | 1 (0.4) | 3 (1.1) | |
| Economic status | |||||
| Low | 259 (11.4) | 195 (10.2) | 16 (12.4) | 48 (17.7) | <0.0011 |
| Medium low | 601 (24.8) | 484 (24.3) | 43 (31.7) | 74 (24.9) | |
| Medium high | 875 (33.9) | 750 (34.9) | 41 (28.4) | 84 (30.8) | |
| High | 783 (29.8) | 661 (30.6) | 45 (27.6) | 77 (26.6) | |
| Insurance | |||||
| Yes | 2,390 (94.0) | 2,001 (95.2) | 134 (96.4) | 255 (88.1) | 0.0082 |
| No | 23 (1.1) | 13 (0.6) | 2 (0.2) | 8 (3.2) | |
| Medical care | 105 (4.9) | 76 (4.2) | 9 (3.4) | 20 (8.7) | |
| Urine cotinine, median [IQR] (ng/mL) | 0.9 [0.4-2.5] | 0.7 [0.4-1.3] | 8.3 [6.3-15.8] 786.5 | [427.7-1,052.6] | <0.001 |
| Residence type | |||||
| General | 914 (41.4) | 716 (38.1) | 73 (59.5) | 125 (51.8) | <0.0011 |
| Apartment | 1,604 (58.6) | 1,374 (61.9) | 72 (40.5) | 158 (48.2) | |
| Residence area | |||||
| Urban | 2,156 (85.5) | 1,811 (86.5) | 116 (76.0) | 229 (83.8) | <0.0011 |
| Rural | 362 (14.5) | 279 (13.5) | 29 (24.0) | 54 (16.2) | |
| Education | |||||
| Father | |||||
| Elementary school | 37 (1.8) | 25 (1.6) | 3 (1.3) | 9 (3.1) | <0.0011 |
| Middle school | 138 (6.0) | 105 (5.1) | 9 (5.5) | 24 (11.6) | |
| High school | 645 (25.8) | 525 (25.6) | 39 (23.7) | 81 (27.8) | |
| College | 878 (32.7) | 787 (36.1) | 34 (22.0) | 57 (18.6) | |
| Not answered | 820 (33.7) | 648 (31.6) | 60 (47.5) | 112 (38.9) | |
| Mother | |||||
| Elementary school | 39 (1.8) | 21 (1.1) | 5 (2.8) | 13 (5.6) | <0.0011 |
| Middle school | 97 (4.3) | 71 (3.9) | 6 (4.4) | 20 (7.0) | |
| High school | 1,072 (42.1) | 885 (42.1) | 66 (46.5) | 121 (39.3) | |
| College | 955 (36.6) | 853 (40.2) | 37 (23.7) | 65 (22.4) | |
| Not answered | 355 (15.2) | 260 (12.7) | 31 (22.6) | 64 (25.7) | |
| Hypertension | |||||
| Father | |||||
| No | 1,740 (72.1) | 1,426 (71.6) | 113 (76.6) | 201 (72.8) | <0.0011 |
| Yes | 306 (12.4) | 250 (12.4) | 18 (13.5) | 38 (12.1) | |
| Not answered | 472 (15.5) | 414 (16.0) | 14 (9.9) | 44 (15.1) | |
| Mother | |||||
| No | 1,926 (79.8) | 1,584 (79.6) | 122 (82.5) | 220 (79.8) | <0.0011 |
| Yes | 118 (4.6) | 92 (4.3) | 9 (7.6) | 17 (4.8) | |
| Not answered | 474 (15.6) | 414 (16.1) | 14 (9.9) | 46 (15.4) | |
| Elevated BP3 | 133 (5.1) | 104 (4.8) | 6 (4.1) | 23 (7.5) | <0.0011 |
| Hypertension4 | 84 (3.1) | 71 (3.1) | 2 (3.3) | 11 (2.7) | <0.0011 |
| Characteristics |
Levels of BP |
p-value | ||
|---|---|---|---|---|
| Normal (n=2,301) | Elevated BP (n=133)1 | Hypertension (n=84)2 | ||
| Age (yr) | 15.3±1.7 | 15.6±1.7 | 15.8±1.6 | <0.001 |
| Sex | ||||
| Male | 1,241 (53.9) | 83 (60.5) | 74 (88.6) | <0.0013 |
| Female | 1,060 (46.1) | 50 (39.5) | 10 (11.4) | |
| Body mass index (kg/m2) | 21.3±3.6 | 24.1±4.8 | 25.8±5.3 | <0.001 |
| Normal | 1,841 (80.6) | 86 (63.8) | 30 (30.7) | <0.0013 |
| Overweight | 219 (8.5) | 6 (4.1) | 14 (16.0) | |
| Obese | 241 (10.9) | 41 (32.1) | 40 (53.3) | |
| Family smoking | ||||
| None | 1,343 (56.6) | 82 (58.0) | 40 (44.3) | <0.0013 |
| Smoking | 470 (21.7) | 23 (13.9) | 25 (29.7) | |
| Not answered | 488 (21.7) | 28 (28.1) | 19 (26.1) | |
| Stress | ||||
| High | 667 (29.2) | 26 (21.1) | 11 (19.7) | <0.0014 |
| Medium | 1,623 (70.3) | 106 (78.3) | 73 (80.3) | |
| Not answered | 11 (0.5) | 1 (0.5) | 0 (0.3) | |
| Economic status | ||||
| Low | 241 (11.6) | 15 (10.3) | 3 (7.0) | <0.0013 |
| Medium low | 539 (24.4) | 36 (29.3) | 26 (31.4) | |
| Medium high | 802 (34.1) | 41 (29.1) | 32 (36.1) | |
| High | 719 (30.0) | 41 (31.4) | 23 (25.4) | |
| Insurance | ||||
| Yes | 2,178 (93.6) | 130 (98.0) | 82 (97.0) | <0.0014 |
| No | 22 (1.1) | 1 (1.3) | 0 (0.0) | |
| Medical care | 101 (5.3) | 2 (0.7) | 2 (3.0) | |
| Urine cotinine, median [IQR] (ng/mL) | 0.9 [0.4-2.3] | 1.2 [0.5-3.9] | 0.8 [0.5-2.7] | 0.277 |
| Residence type | ||||
| General | 819 (40.8) | 59 (41.4) | 36 (38.1) | 0.0803 |
| Apartment | 1,482 (59.2) | 74 (58.6) | 48 (61.9) | |
| Residence area | ||||
| Urban | 1,970 (86.5) | 107 (82.0) | 79 (93.8) | <0.0013 |
| Rural | 331 (13.5) | 26 (18.0) | 5 (6.2) | |
| Education | ||||
| Father | ||||
| Elementary school | 37 (2.0) | 0 (0.0) | 0 (0.0) | <0.0013 |
| Middle school | 122 (6.0) | 5 (4.1) | 11 (11.9) | |
| High school | 587 (25.9) | 38 (24.5) | 20 (23.8) | |
| College | 805 (32.7) | 49 (36.5) | 24 (25.6) | |
| Not answered | 750 (33.4) | 41 (34.8) | 29 (38.6) | |
| Mother | ||||
| Elementary school | 36 (1.9) | 0 (0.0) | 3 (3.7) | <0.0013 |
| Middle school | 86 (4.2) | 10 (8.4) | 1 (1.1) | |
| High school | 952 (41.1) | 67 (48.8) | 53 (61.3) | |
| College | 901 (37.8) | 36 (25.9) | 18 (19.1) | |
| Not answered | 326 (15.1) | 20 (16.9) | 9 (14.8) | |
| Hypertension | ||||
| Father | ||||
| No | 1,601 (69.6) | 90 (70.0) | 49 (53.9) | <0.0013 |
| Yes | 270 (11.7) | 16 (14.7) | 20 (27.0) | |
| Not answered | 430 (18.7) | 27 (15.4) | 15 (19.2) | |
| Mother | ||||
| No | 1,769 (80.3) | 91 (73.5) | 66 (79.6) | <0.0013 |
| Yes | 103 (4.3) | 13 (9.8) | 2 (3.5) | |
| Not answered | 429 (15.4) | 29 (16.8) | 16 (19.9) | |
| Exposure status2 |
Elevated blood pressure (n=133)3 |
Hypertension (n=84)4 |
||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 1 | Model 2 | Model 3 | |
| No tobacco exposure (n=2,090) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Any tobacco exposure (n=428)5 | 1.07 (0.50, 2.28) | 1.66 (0.75, 3.65) | 1.93 (0.86, 4.32) | 1.48 (0.59, 3.71) | 2.16 (0.83, 5.63) | 2.35 (0.88, 6.27) |
| Passive tobacco exposure (n=145) | 0.75 (0.22, 2.55) | 0.91 (0.26, 3.17) | 0.90 (0.29, 2.85) | 0.99 (0.24, 4.07) | 1.17 (0.28, 4.92) | 1.11 (0.28, 4.44) |
| Active smoking (n=283) | 1.34 (0.57, 3.18) | 2.32 (0.94, 5.70) | 3.00 (1.14, 7.89) | 1.89 (0.65, 5.51) | 3.03 (1.00, 9.15) | 3.61 (1.13, 11.49) |
SBP, systolic blood pressure; DBP, diastolic blood pressure.
1 Model 1: Unadjusted; Model 2: Adjusted for age and sex; Model 3: Adjusted for age, sex, body mass index, economic status, family smoking status, stress, and family history of hypertension (paternal or maternal).
2 No tobacco exposure was defined as a urine cotinine level below 5 ng/mL; Passive tobacco exposure was defined as a urine cotinine level of at least 5 ng/mL and less than 100 ng/mL; Active smoking was defined as a urine cotinine level of at least 100 ng/mL.
3 Defined as SBP/DBP greater than 120/80 mmHg.
4 Defined as SBP/DBP greater than 130/80 mmHg.
5 The reference category was no tobacco exposure.
| Exposure status2 | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| No tobacco exposure (n=2,090) | 1.0000 (reference) | 1.0000 (reference) | 1.0000 (reference) |
| Passive tobacco exposure (n=145) | 1.0002 (0.9994, 1.0011) | 1.0007 (0.9997, 1.0018) | 1.0009 (0.9996, 1.0022) |
| Active smoking (n=283) | 1.0004 (0.9994, 1.0014) | 1.0008 (0.9997, 1.0020) | 1.0009 (0.9996, 1.0023) |
1 Model 1: Unadjusted; Model 2: Adjusted for age and sex; Model 3: Adjusted for age, sex, body mass index, economic status, family smoking, stress, family history of hypertension-father and mother.
2 No tobacco exposure is defined as urine cotinine level is below 5 ng/mL; Passive tobacco exposure is defined as urine cotinine is greater than or equal to 5 ng/mL and less than 100 ng/mL; Active smoking is defined as urine cotinine is greater than or equal to 100 ng/mL.
- 1. Kim HC, Cho SM, Lee H, Lee HH, Baek J, Heo JE, et al. Korea hypertension fact sheet 2020: analysis of nationwide populationbased data. Clin Hypertens 2021;27:8 https://doi.org/10.1186/s40885-021-00166-2.ArticlePubMedPMC
- 2. Jeon YW, Kim HC. Factors associated with awareness, treatment, and control rate of hypertension among Korean young adults aged 30-49 years. Korean Circ J 2020;50:1077-1091 https://doi.org/10.4070/kcj.2020.0208.ArticlePubMedPMC
- 3. Chen X, Wang Y. Tracking of blood pressure from childhood to adulthood: a systematic review and meta-regression analysis. Circulation 2008;117:3171-3180 https://doi.org/10.1161/CIRCULATIONAHA.107.730366.ArticlePubMedPMC
- 4. Aryanpur M, Yousefifard M, Oraii A, Heydari G, KazempourDizaji M, Sharifi H, et al. Effect of passive exposure to cigarette smoke on blood pressure in children and adolescents: a metaanalysis of epidemiologic studies. BMC Pediatr 2019;19:161 https://doi.org/10.1186/s12887-019-1506-7.ArticlePubMedPMC
- 5. Barker DJ. Fetal origins of coronary heart disease. BMJ 1995;311:171-174 https://doi.org/10.1136/bmj.311.6998.171.ArticlePubMedPMC
- 6. Heydari G, Yousefifard M, Hosseini M, Ramezankhani A, Masjedi MR. Cigarette smoking, knowledge, attitude and prediction of smoking between male students, teachers and clergymen in Tehran, Iran, 2009. Int J Prev Med 2013;4:557-564.PubMedPMC
- 7. Levy RV, Brathwaite KE, Sarathy H, Reidy K, Kaskel FJ, Melamed ML. Analysis of active and passive tobacco exposures and blood pressure in US children and adolescents. JAMA Netw Open 2021;4:e2037936. https://doi.org/10.1001/jamanetworkopen.2020.37936.ArticlePubMedPMC
- 8. Kim BJ, Han JM, Kang JG, Kim BS, Kang JH. Association between cotinine-verified smoking status and hypertension in 167,868 Korean adults. Blood Press 2017;26:303-310 https://doi.org/10.1080/08037051.2017.1344539.ArticlePubMed
- 9. Kim SH, Lee JS. The association of smoking and hypertension according to cotinine-verified smoking status in 25,150 Korean adults. Clin Exp Hypertens 2019;41:401-408 https://doi.org/10.1080/10641963.2018.1489548.ArticlePubMed
- 10. Hikita N, Haruna M, Matsuzaki M, Sasagawa E, Murata M, Yura A, et al. Comparison of knowledge about smoking and passive smoking and urinary cotinine levels in pregnant women and their partners in Mongolia: a cross-sectional study. Asian Pac Isl Nurs J 2019;4:47-56 https://doi.org/10.31372/20190401.1032.ArticlePubMedPMC
- 11. Kweon S, Kim Y, Jang MJ, Kim Y, Kim K, Choi S, et al. Data resource profile: the Korea National Health and Nutrition Examination Survey (KNHANES). Int J Epidemiol 2014;43:69-77 doi: https://doi.org/0.1093/ije/dyt228.ArticlePubMedPMC
- 12. Textor J. Drawing and analyzing causal DAGs with DAGitty. arXiv [Preprint] 2015;[cited 2023 Jun 10]. Available from: https://doi.org/10.48550/arXiv.1508.04633.Article
- 13. Kim JH, Yun S, Hwang SS, Shim JO, Chae HW, Lee YJ, et al. The 2017 Korean National Growth Charts for children and adolescents: development, improvement, and prospects. Korean J Pediatr 2018;61:135-149 https://doi.org/10.3345/kjp.2018.61.5.135.ArticlePubMedPMC
- 14. SRNT Subcommittee on Biochemical Verification. Biochemical verification of tobacco use and cessation. Nicotine Tob Res 2002;4:149-159 https://doi.org/10.1080/14622200210123581.ArticlePubMed
- 15. Seyedzadeh A, Hashemi F, Soleimani A. Relationship between blood pressure and passive smoking in elementary school children. Iran J Pediatr 2012;22:351-356.PubMedPMC
- 16. Simonetti GD, Schwertz R, Klett M, Hoffmann GF, Schaefer F, Wühl E. Determinants of blood pressure in preschool children: the role of parental smoking. Circulation 2011;123:292-298 https://doi.org/10.1161/CIRCULATIONAHA.110.958769.ArticlePubMed
- 17. Jatoi NA, Jerrard-Dunne P, Feely J, Mahmud A. Impact of smoking and smoking cessation on arterial stiffness and aortic wave reflection in hypertension. Hypertension 2007;49:981-985 https://doi.org/10.1161/HYPERTENSIONAHA.107.087338.ArticlePubMed
- 18. Kallio K, Jokinen E, Raitakari OT, Hämäläinen M, Siltala M, Volanen I, et al. Tobacco smoke exposure is associated with attenuated endothelial function in 11-year-old healthy children. Circulation 2007;115:3205-3212 https://doi.org/10.1161/CIRCULATIONAHA.106.674804.ArticlePubMed
- 19. Virdis A, Giannarelli C, Neves MF, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Curr Pharm Des 2010;16:2518-2525 https://doi.org/10.2174/138161210792062920.ArticlePubMed
- 20. Choi S, Kim Y, Park S, Lee J, Oh K. Trends in cigarette smoking among adolescents and adults in South Korea. Epidemiol Health 2014;36:e2014023. https://doi.org/10.4178/epih/e2014023.ArticlePubMedPMC
- 21. Benowitz NL, Jacob PI, Fong I, Gupta S. Nicotine metabolic profile in man: comparison of cigarette smoking and transdermal nicotine. J Pharmacol Exp Ther 1994;268:296-303.PubMed
- 22. Ferrari MF, Raizada MK, Fior-Chadi DR. Nicotine modulates the renin-angiotensin system of cultured neurons and glial cells from cardiovascular brain areas of Wistar Kyoto and spontaneously hypertensive rats. J Mol Neurosci 2007;33:284-293 https://doi.org/10.1007/s12031-007-9006-x.ArticlePubMed
- 23. Grassi G, Seravalle G, Calhoun DA, Bolla GB, Giannattasio C, Marabini M, et al. Mechanisms responsible for sympathetic activation by cigarette smoking in humans. Circulation 1994;90:248-253 https://doi.org/10.1161/01.CIR.90.1.248.ArticlePubMed
- 24. Hashimoto T, Yoneda M, Shimada T, Kurosawa M, Terano A. Intraportal nicotine infusion in rats decreases hepatic blood flow through endothelin-1 and both endothelin A and endothelin B receptors. Toxicol Appl Pharmacol 2004;196:1-10 https://doi.org/10.1016/j.taap.2003.09.004.ArticlePubMed
- 25. McCall C. A smoke-free generation: New Zealand’s tobacco ban. Lancet 2022;399:1930-1931 https://doi.org/10.1016/S0140-6736(22)00925-4.ArticlePubMed
- 26. Korea Disease Control and Prevention Agency. In Korea, smoking causes over 58,000 annual deaths and incurs social and economic costs of more than 12 trillion won! [cited 2023 Mar 15]. Available from: https://www.kdca.go.kr/board/board.es?mid=a20501010000&bid=0015&list_no=718988&cg_code=&act=view&nPage=1# (Korean).
- 27. Kim S, Kim G. The prevalence of smoking and its implications for tobacco control polices in South Korea. Health Welf Policy Forum 2022;5:6-22 (Korean).
- 28. Kang JM, Cha KS, Kim SJ, Bin JH. A study on urinary nicotine & cotinine levels of smokers, non-smokers. Rep Busan Inst Health Environ 2004;14:63-74 (Korean).
- 29. Park SJ, Seo YB, Lee J, Kim SH, Kim CH. Smoking prevalence and factors associated with false reporting in Korean adolescents: the Korea National Health and Nutrition Examination Survey (2016-2020). Korean J Fam Pract 2022;12:375-383 https://doi.org/10.21215/kjfp.2022.12.5.375.Article
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-


- Related articles
-
- Associations of depressive symptoms with lower extremity function and balance in Korean older adults
- Association of plain water intake with self-reported depression and suicidality among Korean adolescents
- The association of pancreatic cancer incidence with smoking status and smoking amount in Korean men

