
Articles
- Page Path
- HOME > Epidemiol Health > Volume 45; 2023 > Article
-
Original Article
Association of group-level segregation with cardiovascular health in older adults: an analysis of data from the Korean Social Life, Health, and Aging Project -
Sung-Ha Lee1*
 , Hyeok-Hee Lee2,3*, Kiho Sung4, Yoosik Youm4, Hyeon Chang Kim2,3
, Hyeok-Hee Lee2,3*, Kiho Sung4, Yoosik Youm4, Hyeon Chang Kim2,3 -
Epidemiol Health 2023;45:e2023041.
DOI: https://doi.org/10.4178/epih.e2023041
Published online: April 4, 2023
1Center for Happiness Studies, Seoul National University, Seoul, Korea
2Department of Preventive Medicine, Yonsei University College of Medicine, Seoul, Korea
3Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea
4Department of Sociology, Yonsei University, Seoul, Korea
- Correspondence: Hyeon Chang Kim Department of Preventive Medicine, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea E-mail: hckim@yuhs.ac
- Co-correspondence: Yoosik Youm Department of Sociology, Yonsei University, 50 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea E-mail: yoosik@yonsei.ac.kr
- *Lee & Lee contributed equally to this work as joint first authors.
© 2023, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
OBJECTIVES
- The adverse health effects of individual-level social isolation (e.g., perceived loneliness) have been well documented in older adults. However, little is known about the impact of collective-level social isolation on health outcomes. We sought to examine the association of group-level segregation with cardiovascular health (CVH) in older adults.
-
METHODS
- From the prospective Korean Social Life, Health, and Aging Project database, we identified 528 community-dwelling older adults who were aged ≥60 years or were married to those aged ≥60 years. Participants who belonged to smaller social groups separate from the major social group were defined as group-level-segregated. The CVH score was calculated as the number of ideal non-dietary CVH metrics (0-6), as modified from the American Heart Association’s Life’s Simple 7. Using ordinal logistic regression models, we assessed cross-sectional and longitudinal associations between group-level segregation and CVH.
-
RESULTS
- Of the 528 participants (mean age, 71.7 years; 60.0% female), 108 (20.5%) were segregated at baseline. In the cross-sectional analysis, group-level segregation was significantly associated with lower odds of having a higher CVH score at baseline after adjusting for socio-demographic factors and cognitive function (odds ratio [OR], 0.64; 95% confidence interval [CI], 0.43 to 0.95). Among 274 participants who completed an 8-year follow-up, group-level segregation at baseline was marginally associated with lower odds of having a higher CVH score at 8 years (OR, 0.49; 95% CI, 0.24 to 1.02).
-
CONCLUSIONS
- Group-level segregation was associated with worse CVH. These findings imply that the social network structure of a community may influence its members’ health status.
- As social beings, humans must maintain social relationships for survival and well-being. A growing body of evidence indicates that insufficient social connections lead to higher mortality, suggesting that social relationships are crucial for health and longevity [1-3]. In particular, social isolation has repeatedly been reported as a risk factor for premature mortality [3-5]. Among the possible mechanisms linking social disconnection to morbidity and mortality, cardiovascular health (CVH) has emerged as a significant mediator through which social relationships might impact health outcomes [6-9]. Previous studies have shown that individuals with a higher level of loneliness or social isolation exhibit greater risks of hypertension, stroke, coronary heart disease, and myocardial infarction [7,8,10]. Given the multifactorial nature of social relationships, holistic and integrative approaches may be required to investigate their impact on health outcomes.
- A substantial number of studies have focused primarily on individual-level social isolation measures (e.g., lack of social contact or perceived loneliness) concerning health outcomes. In contrast, only a few studies have investigated the prognostic implications of group-level segregation [11-14]. In a recent study examining group-level segregation among individuals of the same race within a single village, segregated older adults exhibited significantly worse self-rated health and higher all-cause mortality after 8 years of follow-up [13,14]. Although these studies have raised awareness of the potential health effects of community-level social relationship factors, the mechanisms underlying the association between group-level segregation and health outcomes remain elusive.
- Using the prospective Korean Social Life, Health, and Aging Project (KSHAP) database, which includes information on the complete social network structure of a single village in Korea, we examined (1) the cross-sectional association between group-level segregation and CVH at baseline; (2) temporal changes in group-level segregation status and CVH; and (3) the longitudinal association between group-level segregation and CVH at follow-up.
INTRODUCTION
- Data source
- The KSHAP is a prospective cohort study designed to examine social activity, health-related factors, and aging in Korean older adults. All inhabitants of Township K in Ganghwa Island, Korea who were aged ≥ 60 years or were married to those aged ≥ 60 years were recruited.
- Township K is one of the 12 townships of Ganghwa Island, the fourth largest island in Korea. The township is a rural community located in the northernmost part of the island, which has been connected to the mainland by bridges since 1970. Most of the inhabitants engage in farming, and nearly half are aged over 60 [15]. The cohort has collected information on participants’ social network structure biennially since its first wave in 2011 and conducted health examinations in 2011 (baseline) and 2019 (follow-up).
- Study population
- A total of 860 participants were recruited in the KSHAP at baseline (2011). Of the 860 individuals in the target population, 814 (94.7%) completed an enumeration survey in the first wave of the KSHAP between December 2011 and July 2012. Among them, 698 participants underwent additional health examinations and were included in the KSHAP-health examination cohort [16]. After excluding 169 participants and 1 participant without available data on the Timed Up-and-Go (TUG) test and educational attainment, respectively, the final study cohort comprised 528 participants. For the longitudinal analysis, the analytic sample was further limited to 274 participants who had complete data for the aforementioned variables at both baseline (2011) and follow-up (2019).
- Group-level segregation
- Group-level segregation status was assessed using a complete social network analysis of Township K [13,17]. In summary, social network nodes were constructed using the information from participants naming up to 6 discussion partners who resided in the same town. Next, the “component” referring to a maximally connected subnetwork was constructed as previously described [13,14]. Any pair of individuals could be reachable either directly or indirectly within the same component, whereas individuals belonging to different components were separated and disconnected. Figure 1 depicts the components constructed in Township K; the most significant component to which the majority of the residents belonged included 672 nodes (blue dots). Group-level segregation was defined as belonging to smaller components separate from the major component (orange dots; Figure 1).
- Cardiovascular health score and covariables
- Each participant’s CVH score was calculated as the number of ideal non-dietary CVH metrics (0-6), as modified from the American Heart Association’s Life’s Simple 7 [18]. The 6 CVH metrics included in the score were smoking, body mass index (BMI), blood pressure (BP), fasting glucose, total cholesterol, and physical function. A higher CVH score reflects better CVH status. Smoking status was assessed as never, former, or current smoking; never or former smoking was defined as the ideal smoking status. BMI was calculated by dividing the weight in kilograms by height in meters squared, and a BMI between 18.5 kg/m2 and 22.9 kg/m2 was defined as ideal BMI status. BP was measured using an oscillometric sphygmomanometer after 5 minutes of rest in the sitting position. Three BP measurements were obtained at 1-minute intervals, and the average of the 3 measurements was used as each participant’s BP; an untreated BP < 120/80 mmHg was defined as ideal BP status. Fasting glucose and total cholesterol levels were measured from blood samples collected after an 8-hour fasting period; an untreated fasting glucose level < 100 mg/dL and a total cholesterol level < 200 mg/dL were defined as ideal fasting glucose and total cholesterol status, respectively. We assessed participants’ physical function using the TUG test, as we lacked detailed information on their physical activity levels. During the test, a medical staff measured the time it took for the participants to rise from an armchair, walk a distance of 3 m, turn, walk back to the chair, and sit down [19]; a TUG time < 13.5 seconds was defined as ideal physical function status. The TUG time has been reported as a good predictor of functional mobility and frailty in older adults [20].
- Data on participants’ demographics, educational attainment (elementary school or less, middle school, high school, and college or higher), social network size, marital status (living with a spouse or not), Mini-Mental State Examination for Dementia Screening (MMSE) score, and household income were also collected.
- Statistical analysis
- Baseline characteristics were presented as mean± standard deviation or number (%) and compared using the independent t-test or chi-square test. In the cross-sectional analysis, we examined the association of group-level segregation with the CVH score at baseline using ordinal logistic regression models, treating the CVH score as an ordinal variable from 0 to 6. The “Polr” function of the MASS package in R was used for the analyses. Potential confounders were adjusted stepwise: model 1 included age, sex, and educational attainment; model 2 was further adjusted for social network size and marital status; and model 3 was further adjusted for the MMSE score.
- In the longitudinal analysis, we assessed the temporal changes in group-level segregation status and CVH score among 274 participants who completed an 8-year follow-up. We also investigated the association of group-level segregation at baseline with CVH score at 8 years using the same regression models mentioned above, all of which were further adjusted for the baseline CVH score.
- As sensitivity analyses, we repeated our main regression analyses after further adjusting for household income or depressive symptoms assessed by the Center for Epidemiologic Studies Depression scale in the subset of participants who had available information. All statistical analyses were conducted using R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
- Ethics statement
- This study complied with the Declaration of Helsinki, and the study protocol was approved by the Institutional Review Board of Yonsei University, Seoul, Korea (YUIRB-2011-012-01; 7001988-202111-HR-505-04). Written informed consent was obtained from all participants.
MATERIALS AND METHODS
- Baseline characteristics of the participants
- Of the 528 participants (mean age, 71.7 years; 60.0% female), 108 (20.5%) displayed social segregation at baseline. The segregated individuals were younger, were more highly educated, had smaller social networks, and lived with their spouses less frequently than those who were integrated (Table 1).
- Association of group-level segregation with the cardiovascular health score at baseline
- Group-level segregation was significantly associated with reduced odds of having a higher CVH score at baseline after adjusting for demographics and educational attainment (model 1: odds ratio [OR], 0.65; 95% confidence interval [CI], 0.44 to 0.95). The association remained significant after further adjusting for social network size and marital status (model 2: OR, 0.61; 95% CI, 0.41 to 0.90), and MMSE score (model 3: OR, 0.64; 95% CI, 0.43 to 0.95) (Table 2). The findings were generally consistent when we additionally adjusted for household income (n=431; OR, 0.69; 95% CI, 0.43 to 1.11) or depressive symptoms (n=521; OR, 0.64; 95% CI, 0.44 to 0.96) in the sensitivity analyses.
- Temporal changes in group-level segregation status and cardiovascular health score
- Of the 274 participants (mean age, 69.7 years; 61.7% female) who completed an 8-year follow-up, 34 (12.4%) showed social segregation at baseline (Supplementary Material 1). Similar to the participants in cross-sectional analysis, the segregated individuals were younger and more highly educated than integrated individuals. However, the 2 groups did not differ regarding social network size, marital status, or cognitive function (Supplementary Material 1).
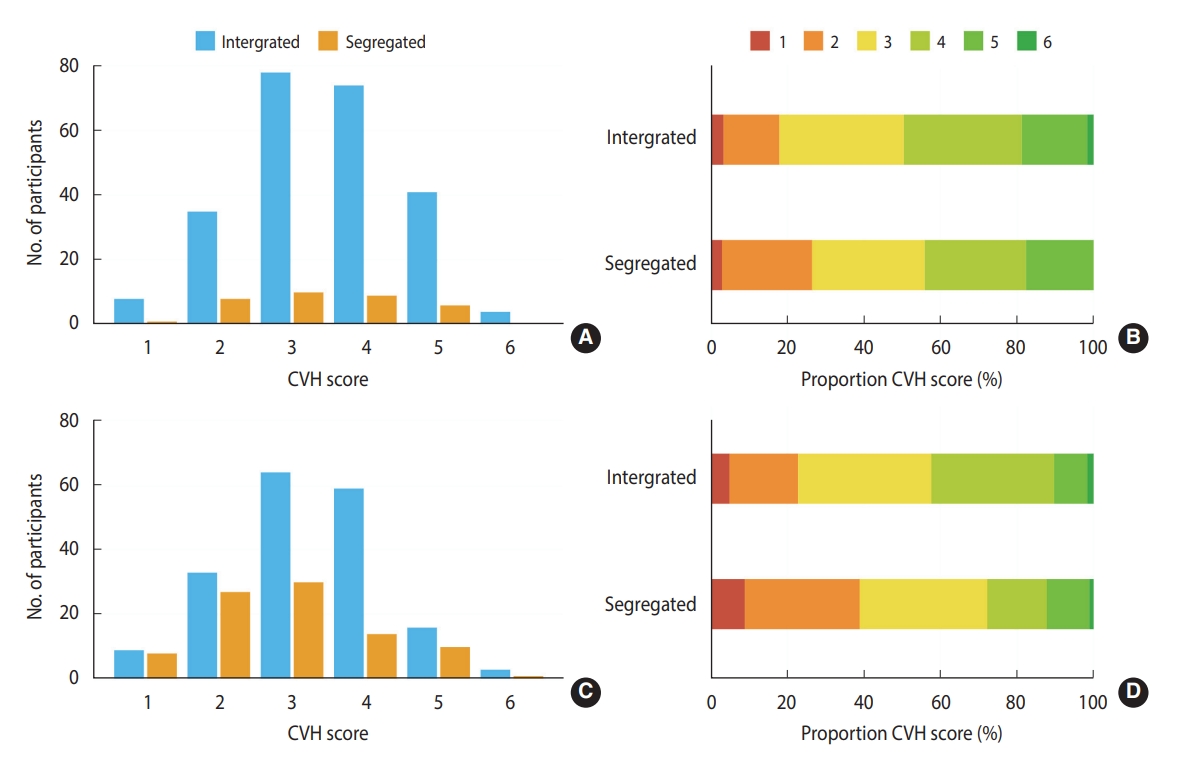
- Over the follow-up, the proportion of segregated individuals increased from 12.4% to 32.8% (p<0.001; Table 3), and the CVH score decreased, remained the same, and increased in 40.1%, 37.6%, and 22.3% of the participants, respectively (Figure 2 and Table 3). When each metric was analyzed separately, the proportion of participants with ideal fasting glucose decreased from 76.3% to 66.4% (p=0.011), and that of participants with ideal physical function decreased from 74.8% to 58.0% (p<0.001; Table 3). The distribution of CVH scores at baseline and at 8 years among those who completed the follow-up is described in Figure 3.
- Association of group-level segregation at baseline with cardiovascular health score at follow-up
- Group-level segregation at baseline was marginally associated with reduced odds of having a higher CVH score at 8 years after adjusting for baseline CVH score, demographics, educational attainment, social network size, marital status, and MMSE score (model 3: OR, 0.49, 95% CI, 0.24 to 1.02) (Table 4). The findings were broadly similar when we additionally adjusted for household income (n=231; OR, 0.44; 95% CI, 0.18 to 1.06) or depressive symptoms (n=270; OR, 0.50, 95% CI, 0.23 to 1.02) in the sensitivity analyses.
RESULTS
- This prospective cohort study showed that community-level social isolation was significantly associated with worse CVH among Korean older adults. Segregated participants within small groups whose network did not reach the whole village exhibited worse CVH profiles than those who were integrated. Moreover, this negative association between group-level segregation and CVH persisted after 8 years, implying that socially isolated individuals, in general, remained unhealthy unless they were specially cared for or received an intervention of some sort. The associations of group-level segregation with individual CVH metrics varied to some extent, especially for smoking and total cholesterol (Supplemental Material 2). However, the analyses were largely underpowered to draw any definitive conclusions.
- Our findings are in accordance with previous studies demonstrating the associations of neighborhood-level segregation with cardiovascular diseases and mortality [21-23]. However, those studies primarily focused on African Americans and investigated how racial or ethnic residential segregation contributed to health disparities. Non-social differences between races or ethnicities (e.g., genetic predisposition and racial discrimination) may have contributed to the relationship between segregation and health outcomes. Further evidence on the direct connection between social aspects of segregation and an individual’s health status has therefore been warranted.
- The present study focused on whether group-level segregation in a homogeneous ethnic group can impact health outcomes. Utilizing a single racial group and complete social network structure of an entire town, we showed that group-level segregation was associated with worse CVH at both baseline and 8 years. Herein, we speculate that 2 possible pathways might link group-level segregation and CVH. First, segregated older adults may be less likely to have access to communication resources disseminated through local community networks, which may restrict their ability to obtain sufficient health information for maintaining ideal CVH. Among racially segregated African Americans and Latinos in the United States, limited access to community-based communication infrastructure was associated with a reduced chance of obtaining knowledge about the detection and prevention of chronic diseases [24]. In this light, encouraging segregated older adults to engage in community-level programs, including local walking groups and community organization-based exercise, might be an effective intervention for promoting CVH [25,26]. This appears to be a viable approach, given that nearly 70% of Korean older adults in rural areas regularly attend senior community centers that offer social and recreational activities as well as health and wellness programs [27]. The finding that segregated older adults were younger and more educated than their integrated counterparts also renders such an approach more feasible. Second, social segregation can increase the level of psychological distress, which is a significant risk factor for poor CVH. Previous studies have suggested that psychological stress may, at least partly, mediate the association between the level of segregation and blood pressure [23,28]. It can be argued that segregated individuals may lack a sense of belonging to the community or lack community-level social support, which can elevate stress levels and subsequently lead to an increased risk of cardiovascular disease [29,30].
- A growing body of evidence has linked health outcomes with individual-level social disconnection, such as loneliness, which is a subjective experience of social isolation [10,31-33]. However, less attention has been paid to the impact of group-level or society-level isolation on individuals’ health outcomes. The present study extends the existing literature by exploring the potential impact of community-level social relationship factors obtained from social network analysis on CVH profiles. Taken together with the recent finding that group-level segregation is a strong predictor of mortality [13], our results imply that CVH may be a potential mediator between segregation and mortality. However, a mechanistic understanding of the observed findings will require further comprehensive investigations, which should include social, structural, and functional factors that determine social connection or health status [31,34].
- Our findings should be interpreted in light of several limitations. First, a causal relationship between group-level segregation and worse CVH could not be established due to the observational nature of the study. Second, despite adjusting for major covariables, including demographic characteristics, social factors, and cognitive function, the possibility of residual confounding still exists. In particular, unmeasured confounders, such as nutritional intake, physical activity, and genetic predisposition, may have affected the association between group-level segregation and CVH. Third, given the cohort’s low retention rate (52%) over the follow-up, we cannot exclude the possibility of selection bias in our longitudinal analysis. As a matter of fact, the participants who completed the follow-up were significantly younger and, interestingly, less segregated than those who were lost to follow-up (Supplemental Material 3). It is possible that group-level segregation was a factor that influenced the retention rate. Fourth, although group-level segregation was consistently associated with worse CVH in various analyses, its associations with individual CVH metrics varied to some extent. Further research is needed to firmly establish the impact of group-level segregation on each CVH metric. Fifth, each component of the CVH score may have a differential influence on cardiovascular disease risk. However, as the main purpose of the CVH score is to monitor how well an individual or a population manages their cardiovascular risk profile rather than predicting the absolute risk of developing cardiovascular disease, we focused on the number of ideal CVH metrics without considering the differential impact of each component [18]. Finally, the study cohort was composed entirely of Korean older adults; whether the findings can be generalized to other ethnic or racial populations or age groups should be determined in future studies.
- In older adults, group-level segregation was associated with worse CVH at both baseline and 8 years. These findings underscore the importance of community-level social isolation as one of the potential determinants of an individual’s health status that should be considered when developing future health promotion interventions for older adults. Further studies are warranted to demonstrate the potential mechanisms by which group-level segregation affects an individual’s health outcomes.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2022S1A3A2A02089737).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Lee SH, Lee HH, Sung K. Formal analysis: Lee SH, Lee HH. Funding acquisition: Kim HC, Youm Y. Methodology: Lee SH, Lee HH, Sung K. Project administration: Sung K. Visualization: Lee SH, Lee HH. Writing – original draft: Lee SH, Lee HH. Writing – review & editing: Lee SH, Lee HH, Sung K, Youm Y, Kim HC.
NOTES
ACKNOWLEDGEMENTS



| Characteristics | Total (n=528) | Integrated (n=420) | Segregated (n=108) | p-value | |
|---|---|---|---|---|---|
| Age (yr) | 71.7±7.4 | 72.0±7.0 | 70.3±8.4 | 0.025 | |
| Sex | 0.360 | ||||
| Male | 211 (40.0) | 172 (41.0) | 39 (36.1) | ||
| Female | 317 (60.0) | 248 (59.0) | 69 (63.9) | ||
| Educational attainment | 0.011 | ||||
| Elementary school or less | 168 (31.8) | 144 (34.3) | 24 (22.2) | ||
| Middle school | 223 (42.2) | 174 (41.4) | 49 (45.4) | ||
| High school | 71 (13.4) | 58 (13.8) | 13 (12.0) | ||
| College or higher | 66 (12.5) | 44 (10.5) | 22 (20.4) | ||
| Social network size | 3.2±1.3 | 3.3±1.3 | 2.8±1.2 | <0.001 | |
| Marital status | 0.044 | ||||
| Living with a spouse | 392 (74.2) | 320 (76.2) | 72 (66.7) | ||
| Living without a spouse1 | 136 (25.8) | 100 (23.8) | 36 (33.3) | ||
| MMSE score | 24.0±4.6 | 24.2±4.1 | 23.3±6.1 | 0.068 | |
| Household income (US$/yr) | 0.952 | ||||
| <10,000 | 288/431 (66.8) | 239/358 (66.8) | 49/73 (67.1) | ||
| ≥10,000 | 143/431 (33.2) | 119/358 (33.2) | 24/73 (32.9) | ||
| CVH score | 0.369 | ||||
| 6 | 9 (1.7) | 9 (2.1) | 0 (0.0) | ||
| 5 | 79 (15.0) | 66 (15.7) | 13 (12.0) | ||
| 4 | 152 (28.8) | 123 (29.3) | 29 (26.9) | ||
| 3 | 169 (32.0) | 130 (31.0) | 39 (36.1) | ||
| 2 | 96 (18.2) | 76 (18.1) | 20 (18.5) | ||
| 1 | 23 (4.4) | 16 (3.8) | 7 (6.5) | ||
Values are presented as mean±standard deviation for continuous variables and number (%) for categorical variables.
CVH, cardiovascular health; MMSE, Mini-Mental State Examination for Dementia Screening.
1 Including participants who were widowed (n=133) or separated (n=1), or who never married (n=2).
Values are presented as odds ratio (95% confidence interval).
CVH, cardiovascular health; MMSE, Mini-Mental State Examination for Dementia Screening.
1 All covariables were collected or measured at baseline.
2 Model 1 was adjusted for baseline CVH score, age, sex, and educational attainment; Model 2 was further adjusted for social network size and marital status; Model 3 was further adjusted for the MMSE score.
- 1. Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci 2015;10:227-237.ArticlePubMedPDF
- 2. Luo Y, Hawkley LC, Waite LJ, Cacioppo JT. Loneliness, health, and mortality in old age: a national longitudinal study. Soc Sci Med 2012;74:907-914.ArticlePubMedPMC
- 3. O’Súilleabháin PS, Gallagher S, Steptoe A. Loneliness, living alone, and all-cause mortality: the role of emotional and social loneliness in the elderly during 19 years of follow-up. Psychosom Med 2019;81:521-526.ArticlePubMedPMC
- 4. Abell JG, Steptoe A. Living alone and mortality: more complicated than it seems. Eur Heart J Qual Care Clin Outcomes 2019;5:187-188.ArticlePubMed
- 5. Jensen MT, Marott JL, Holtermann A, Gyntelberg F. Living alone is associated with all-cause and cardiovascular mortality: 32 years of follow-up in the Copenhagen Male Study. Eur Heart J Qual Care Clin Outcomes 2019;5:208-217.ArticlePubMed
- 6. Hodgson S, Watts I, Fraser S, Roderick P, Dambha-Miller H. Loneliness, social isolation, cardiovascular disease and mortality: a synthesis of the literature and conceptual framework. J R Soc Med 2020;113:185-192.ArticlePubMedPMCPDF
- 7. Hakulinen C, Pulkki-Råback L, Virtanen M, Jokela M, Kivimäki M, Elovainio M. Social isolation and loneliness as risk factors for myocardial infarction, stroke and mortality: UK Biobank cohort study of 479 054 men and women. Heart 2018;104:1536-1542.ArticlePubMed
- 8. Valtorta NK, Kanaan M, Gilbody S, Ronzi S, Hanratty B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: systematic review and meta-analysis of longitudinal observational studies. Heart 2016;102:1009-1016.ArticlePubMed
- 9. Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med 2010;40:218-227.ArticlePubMed
- 10. Cacioppo JT, Ernst JM, Burleson MH, McClintock MK, Malarkey WB, Hawkley LC, et al. Lonely traits and concomitant physiological processes: the MacArthur social neuroscience studies. Int J Psychophysiol 2000;35:143-154.ArticlePubMed
- 11. Kramer MR, Hogue CR. Is segregation bad for your health? Epidemiol Rev 2009;31:178-194.ArticlePubMed
- 12. Acevedo-Garcia D, Lochner KA, Osypuk TL, Subramanian SV. Future directions in residential segregation and health research: a multilevel approach. Am J Public Health 2003;93:215-221.ArticlePubMedPMC
- 13. Youm Y, Baldina E, Baek J. All-cause mortality and three aspects of social relationships: an eight-year follow-up of older adults from one entire Korean village. Sci Rep 2021;11:465.ArticlePubMedPMCPDF
- 14. Youm Y, Sung K. Self-rated health and global network position: results from the older adult population of a Korean rural village. Ann Geriatr Med Res 2016;20:149-159.ArticlePDF
- 15. Youm Y, Laumann EO, Ferraro KF, Waite LJ, Kim HC, Park YR, et al. Social network properties and self-rated health in later life: comparisons from the Korean social life, health, and aging project and the national social life, health and aging project. BMC Geriatr 2014;14:102.ArticlePubMedPMCPDF
- 16. Lee JM, Lee WJ, Kim HC, Choi W, Lee J, Sung K, et al. The Korean social life, health and aging project-health examination cohort. Epidemiol Health 2014;36:e2014003.ArticlePubMedPMC
- 17. Wasserman S, Faust K. Social network analysis: methods and applications. Cambridge: Cambridge University Press; 1994. p 92-166.
- 18. Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010;121:586-613.ArticlePubMed
- 19. Podsiadlo D, Richardson S. The Timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991;39:142-148.ArticlePubMed
- 20. Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go test. Phys Ther 2000;80:896-903.ArticlePubMedPDF
- 21. Kershaw KN, Osypuk TL, Do DP, De Chavez PJ, Diez Roux AV. Neighborhood-level racial/ethnic residential segregation and incident cardiovascular disease: the multi-ethnic study of atherosclerosis. Circulation 2015;131:141-148.ArticlePubMed
- 22. Kershaw KN, Albrecht SS. Racial/ethnic residential segregation and cardiovascular disease risk. Curr Cardiovasc Risk Rep 2015;9:10.ArticlePubMedPMCPDF
- 23. Kershaw KN, Robinson WR, Gordon-Larsen P, Hicken MT, Goff DC Jr, Carnethon MR, et al. Association of changes in neighborhood-level racial residential segregation with changes in blood pressure among Black adults: the CARDIA Study. JAMA Intern Med 2017;177:996-1002.ArticlePubMedPMC
- 24. Kim YC, Moran MB, Wilkin HA, Ball-Rokeach SJ. Integrated connection to neighborhood storytelling network, education, and chronic disease knowledge among African Americans and Latinos in Los Angeles. J Health Commun 2011;16:393-415.ArticlePubMed
- 25. Schwarte L, Samuels SE, Capitman J, Ruwe M, Boyle M, Flores G. The Central California Regional Obesity Prevention Program: changing nutrition and physical activity environments in California’s heartland. Am J Public Health 2010;100:2124-2128.ArticlePubMedPMC
- 26. Yanek LR, Becker DM, Moy TF, Gittelsohn J, Koffman DM. Project Joy: faith based cardiovascular health promotion for African American women. Public Health Rep 2001;116(Suppl 1):68-81.ArticlePubMedPMCPDF
- 27. Park KS, Park YR, Yum YS. Who is not going to Gyungrodang in rural areas? Soc Welf Policy 2015;42:163-184 (Korean).Article
- 28. Kershaw KN, Diez Roux AV, Burgard SA, Lisabeth LD, Mujahid MS, Schulz AJ. Metropolitan-level racial residential segregation and black-white disparities in hypertension. Am J Epidemiol 2011;174:537-545.ArticlePubMedPMC
- 29. Wirtz PH, von Känel R. Psychological stress, inflammation, and coronary heart disease. Curr Cardiol Rep 2017;19:111.ArticlePubMedPDF
- 30. Rohleder N. Stimulation of systemic low-grade inflammation by psychosocial stress. Psychosom Med 2014;76:181-189.ArticlePubMed
- 31. Holt-Lunstad J. Why social relationships are important for physical health: a systems approach to understanding and modifying risk and protection. Annu Rev Psychol 2018;69:437-458.ArticlePubMed
- 32. Eisenberger NI, Moieni M, Inagaki TK, Muscatell KA, Irwin MR. In sickness and in health: the co-regulation of inflammation and social behavior. Neuropsychopharmacology 2017;42:242-253.ArticlePubMedPDF
- 33. Lee SH, Cole SW, Park J, Choi I. Loneliness and immune gene expression in Korean adults: the moderating effect of social orientation. Health Psychol 2021;40:686-691.ArticlePubMed
- 34. Slavich GM. Social safety theory: a biologically based evolutionary perspective on life stress, health, and behavior. Annu Rev Clin Psychol 2020;16:265-295.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Association of social isolation and loneliness with the risk of hypertension in middle aged and older adults: Findings from a national representative longitudinal survey
Shiqi Wang, Hao Zhang, Yiling Lou, Qiqi You, Qingqing Jiang, Shiyi Cao
Journal of Affective Disorders.2024; 349: 577. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite




