Articles
- Page Path
- HOME > Epidemiol Health > Volume 44; 2022 > Article
-
Original Article
Dairy product consumption and type 2 diabetes among Korean adults: a prospective cohort study based on the Health Examinees (HEXA) study -
Jiaqi Zhang1
 , Kyungjoon Lim2, Sangah Shin1
, Kyungjoon Lim2, Sangah Shin1 -
Epidemiol Health 2022;44:e2022019.
DOI: https://doi.org/10.4178/epih.e2022019
Published online: February 4, 2022
1Department of Food and Nutrition, Chung-Ang University, Anseong, Korea
2Faculty of Medicine and Health, School of Medical Science, University of Sydney, Melbourne, Australia
- Correspondence: Sangah Shin Department of Food and Nutrition, Chung-Ang University, 4726 Seodong-daero, Anseong 17546, Korea E-mail: ivory8320@cau.ac.kr
©2022, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
OBJECTIVES
- It has been suggested that the consumption of dairy products helps lower the prevalence of type 2 diabetes (T2D). We investigated the association between the consumption of dairy products and T2D events in middle-aged Korean adults.
-
METHODS
- We followed up 53,288 participants (16,895 male and 36,393 female) in the Health Examinees (HEXA) study. The consumption of dairy products was assessed using the self-administered food frequency questionnaire, and T2D was defined according to the 2015 treatment guidelines of the Korean Diabetes Association. Hazard ratios (HRs) and 95% confidence intervals (CIs) between the consumption of dairy products and the risk of T2D were calculated using Cox proportional hazards models after adjusting for potential confounders. Spline regression was used to better represent the association between the consumption of dairy products and the risk of T2D.
-
RESULTS
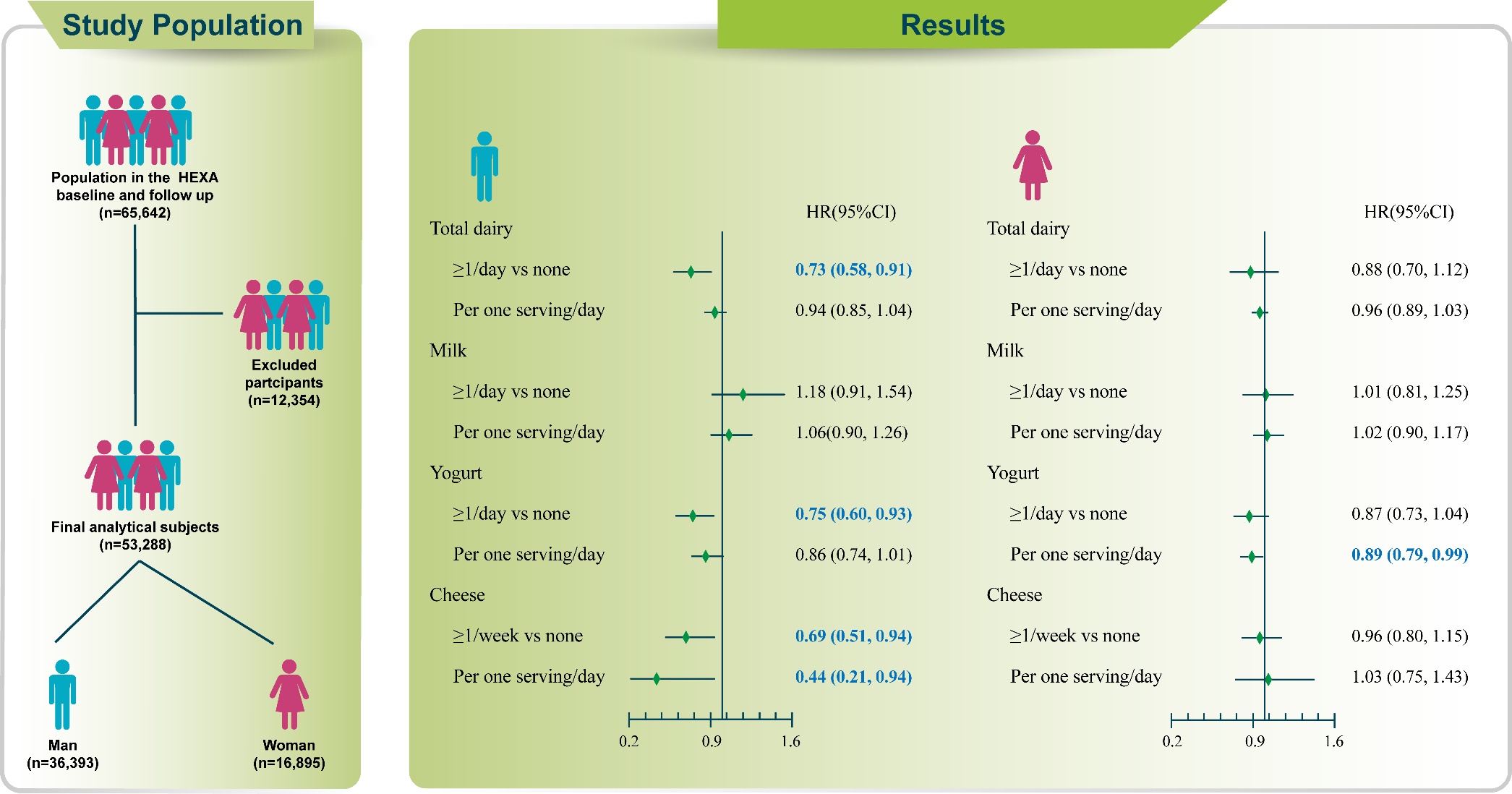
- Among male, those with higher consumption of dairy products had a significantly lower risk of T2D than those who consumed essentially no dairy products (HR, 0.73; 95% CI, 0.58 to 0.91). In particular, consumption of yogurt (HR, 0.75; 95% CI, 0.60 to 0.93; ptrend=0.035) and cheese (HR, 0.66; 95% CI, 0.49 to 0.89; ptrend=0.005) was negatively associated with the incidence of T2D in male. In female, daily consumption of 1 serving of yogurt decreased the risk of T2D by 11%.
-
CONCLUSIONS
- The association between the consumption of dairy products and the risk of T2D differed by sex and dairy product type. Further prospective studies are needed to confirm these associations.
- Type 2 diabetes (T2D) is among the most prevalent chronic diseases worldwide, with 9.3% of adults (around 463 million) living with the condition [1], and its incidence is increasing. The International Diabetes Federation projects that approximately 578 million adults will have T2D by 2030 [2]. Diabetes is a disease of concern in Korea; in 2020, T2D was prevalent in 13.8% of adults (approximately 4.94 million) aged over 30 years [3]. T2D is a serious chronic disease caused by a complex combination of genetic and environmental interaction and other risk factors such as lifestyle [4]. Thus, it is important to understand the modifiable factors associated with the risk of T2D.
- One of these modifiable risk factors is diet, in particular, dairy products. Dairy products contain saturated fat, which is generally considered to have adverse effects on health [5]. Excessive intake of saturated fat increases the risk of cardiovascular disease [6]. Regular consumption of milk protein causes the insulin-like growth factor-1 (IGF-1) axis to permanently increase serum IGF-1 levels. Insulin/IGF-1 signaling is closely linked to the development of chronic diseases such as T2D, obesity, and cancer [7]. However, there is also increasing evidence supporting a possible benefit of dairy products in the management of T2D. Dairy products contain calcium, vitamin D, whey protein, and flavonoids, which have a favorable effect on glucose homeostasis and thus improve T2D [8,9]. In addition, the lactic acid bacteria found in fermented dairy products, such as yogurt and cheese, contribute to intestinal microbial balance [10], which may improve T2D by reducing the risk of obesity [11].
- In several studies, dairy products were divided into milk, yogurt, and cheese [12-14]. A large cohort study of Chinese adults found that daily milk intake was associated with a significant reduction in the risk of T2D [15]. A study on yogurt intake and the risk of diabetes, which evaluated 3 cohorts of the United States adults, found that increased yogurt intake was associated with a reduced risk of T2D [16]. In the European Prospective Investigation into Cancer and Nutrition study, a negative association between diabetes and cheese intake was found [17]. However, most of these studies were focused on the association between dairy product intake and the risk of T2D in Western countries. Furthermore, most current studies on dairy consumption and T2D in Korea are cross-sectional studies [18] with inadequate data [19]. The variety of dairy products and dairy product intake are lower in Korea than in Western countries [12,13,20]. Therefore, cohort studies on the association between the consumption of dairy products and the risk of T2D in Korea are limited.
- Given the increasing incidence of T2D among Koreans [3], it is crucial to understand the significance of the consumption of dairy products for the prevention of T2D. Thus, this study aimed to investigate the effect of consumption of dairy products, including milk, yogurt, and cheese, on the incidence of T2D among Korean adults aged 40-69 years, using data from a large Korean population.
INTRODUCTION
- Study population
- The Health Examinees (HEXA) study was a part of the Korean Genome and Epidemiology Study, a large, prospective, community-based genomic cohort study. The HEXA study was conducted to investigate the cause of major chronic diseases in Koreans [21]. The baseline survey for the HEXA study was conducted from 2004 to 2013 at 38 hospitals and local health screening centers following strict standardized study procedures. In total, 65,642 participants completed the initial and follow-up surveys between 2012 and 2016 [21].
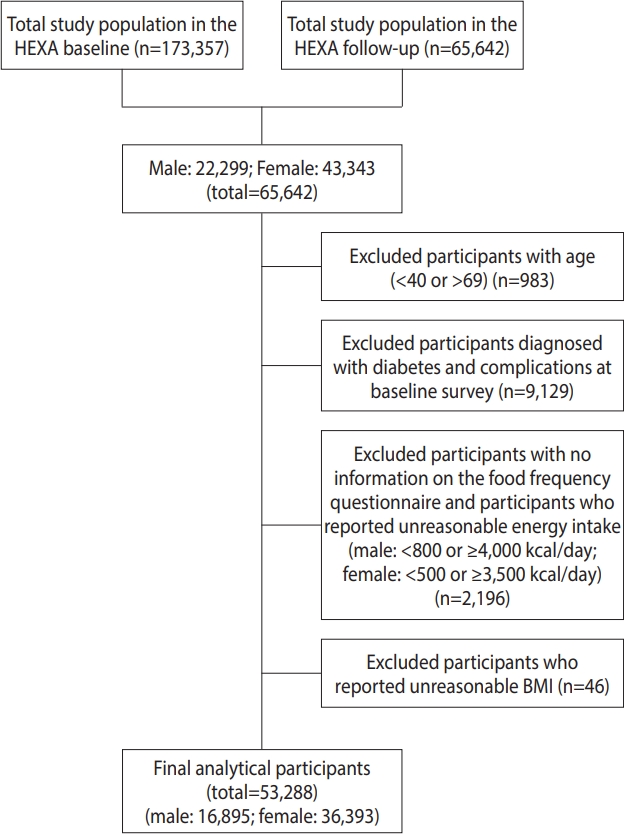
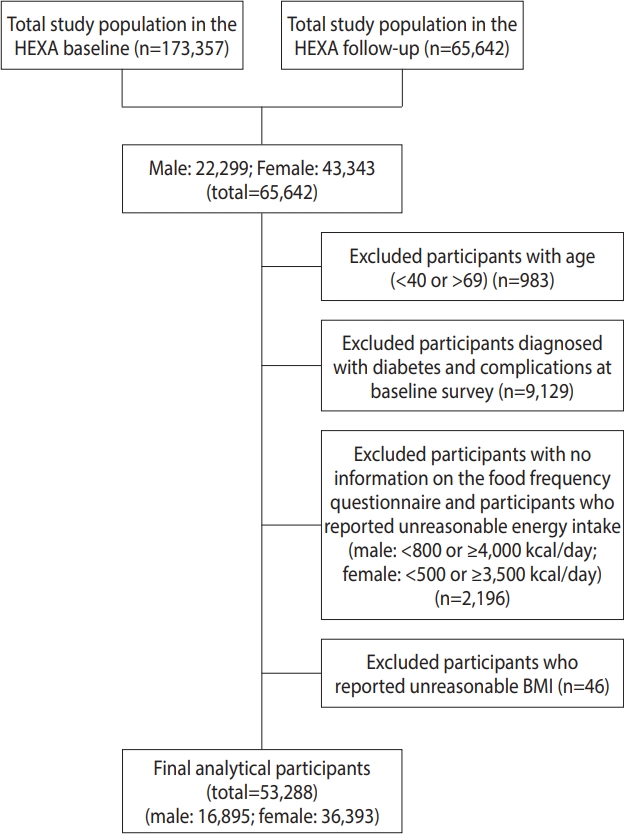
- Among the 65,642 participants who completed the baseline and follow-up surveys, we excluded those aged < 40 years and > 69 years (n = 983) and those who were diagnosed with T2D and complications at the baseline survey (n = 9,129). Further, we excluded those without dietary intake records or those who reported an unreasonable amount of energy intake ( < 800 or ≥ 4,000 kcal/day in male and < 500 or ≥ 3,500 kcal/day in female; n= 2,196). Participants with missing information on body mass index (BMI; n= 46) were also excluded. Finally, 53,288 participants (16,895 male and 36,393 female) were included in the final analysis (Figure 1).
- Assessment of dairy product consumption
- Food intake in the past year was assessed using a 106-item selfadministered food frequency questionnaire (FFQ). The frequency of food consumption was classified into 9 categories: never or almost never, once a month, 2 to 3 times a month, once or twice a week, 3 to 4 times a week, 5 to 6 times a week, once a day, twice a day, and 3 times a day. The portion sizes were categorized into 3 groups: half standard serving, 1 standard serving, and 2 standard servings. The dairy products in the FFQ included 3 types: milk, yogurt, and cheese. One serving size was equal to 200 mL for milk, 120 mL for yogurt, and 20 g for cheese. The consumption of dairy products was converted to a weekly frequency and multiplied by the number of servings reported for each food. Based on their reported distribution of each target dairy product, the participants were categorized into 3 groups for consumption of cheese (none, < 1, and ≥ 1/wk) and 4 groups for consumption of dairy products, milk, and yogurt (none, ≤ 2, > 2-< 7/wk, and ≥ 1/day).
- To verify the validity and 1-year repeatability of the FFQ, information was collected in each of the 4 seasons of the 1-year period using the 3-day diet record method. The correlation coefficients between the FFQ and 12-day diet record, adjusted for attenuation, age, sex, and energy intake in the Korean population, ranged between 0.23 and 0.64, with 0.45 being the value for nutrient intake and 0.39 for nutrient density [22].
- Definition of type 2 diabetes
- T2D was defined according to the 2015 treatment guidelines of the Korean Diabetes Association as a fasting blood glucose level ≥ 126 mg/dL or active treatment with glucose-lowering medication (insulin or oral hypoglycemic agents), at a follow-up survey [23]. The number of person-years was calculated by multiplying the average number of participants by the number of years of observation.
- Covariates
- Covariates included socio-demographic factors such as age, BMI, educational level, and health behavior. Education levels were divided into 3 categories: middle school or less, high school or college, and undergraduate school or higher. Smoking status was assessed using the question “Have you smoked 5 packs of cigarettes (100 cigarettes) in your lifetime?” Participants who answered “no” were defined as non-smokers. Meanwhile, those who answered “yes” were categorized as current smokers or ever-smokers if they still smoked or no longer smoked at the time of the survey, respectively. Drinking status was determined by the question “Are you unable to drink alcohol or do you choose not to drink alcohol?” Participants who answered “no” were identified as non-drinkers, while those who answered “yes” were classified as current drinkers. Physical activity was assessed with the question “Do you regularly participate in any sport?” Participants who answered “yes” were assigned to the regular exercise group, while those who answered “no” were assigned to the non-regular exercise group.
- Statistical analysis
- All analyses to investigate the association between the consumption of dairy products and the risk of T2D were conducted separately by sex. Categorical variables were analyzed using the chisquare test, while continuous variables were analyzed using general linear regression. The association between consumption of dairy products and the development of T2D was determined by calculating hazard ratios (HRs) and 95% confidence intervals (CIs) using Cox proportional hazard models. We used multivariate models adjusted for age, BMI, educational level (≤ middle school, high school or college, undergraduate school or higher), smoking status (never, ever, current, unknown), alcohol drinking status (never, ever, unknown), physical activity (yes, no, unknown), and total energy intake as covariates. To test for a linear trend between the consumption of dairy products and HR for T2D, participants were assigned a median value for each category, and this variable was entered into the model as a continuous term. The coefficient was assessed using the Wald test. To assess the linearity of the association between the consumption of dairy products and the risk of T2D, we used spline regression analysis. Constrained cubic splines were fitted to logistic and proportional risk regression models to non-parametrically examine the relationship between the consumption of dairy products and the HR for T2D, with 4 knots at fixed percentiles (5th, 35th, 65th, and 95th percentiles). We used the restricted maximum likelihood method in our analysis, combining the 2 regression coefficients and variance matrices estimated in this study. The pooled relative risk for a given exposure value was then estimated. The p-values for non-linearity were calculated by testing the null hypothesis that the coefficients of the second spline were equal to 0. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). A p-value ≤ 0.05 was considered to indicate statistical significance.
- Ethics statement
- All participants voluntarily signed an informed written consent form prior to enrollment. The current study was performed in accordance with the guidelines specified in the declaration of Helsinki, and the study protocol was approved by the local Institutional Review Board (IRB) of the Ethics Committee of the Korean Genome and Epidemiology Study of the Korea National Institute of Health (IRB No. 2014-08-02-3C_A).
MATERIALS AND METHODS
- The characteristics of the participants according to the consumption of dairy products are shown in Table 1. Compared with male who consumed no or less dairy products every week, those who consumed dairy products once or more per day were younger, with higher education levels, and were more likely to perform regular exercise. Similarly, female who consumed dairy products at least once a day were younger, had higher education levels, were less likely to be smokers, and were regular exercisers. Both male and female with a higher consumption of dairy products also consumed higher amounts of energy, carbohydrates, protein, and fat. The trends in the characteristics of the participants according to their consumption of milk, yogurt, and cheese were similar to those according to the total consumption of dairy products (Supplementary Materials 1-3).
- Table 2 shows the multivariate HRs (95% CI) for T2D according to the consumption of total dairy products, milk, yogurt, and cheese. Among male, those who consumed dairy products, including yogurt and cheese, had a lower risk of T2D than those who did not consume dairy products. In the comparison between the highest and lowest (non)-intake categories, the multivariate HRs (95% CIs) for the consumption of total dairy products, yogurt, and cheese were 0.73 (95% CI, 0.58 to 0.91), 0.75 (95% CI, 0.60 to 0.93), and 0.69 (95% CI, 0.51 to 0.94), respectively. However, in dairy products, the p for trend was not significant. In female, there was no significant association for the consumption of total dairy products, milk, yogurt, and cheese. However, increasing the consumption of yogurt by 1 serving/day may reduce the risk of T2D by 11% (HR, 0.89; 95% CI, 0.79 to 0.99).
- Spline regression was used to better characterize the association between the consumption of dairy products and the risk of T2D. As shown in Figure 2, the 4 knots of the consumption of dairy products for male were 0.00, 1.44, 4.29, and 12.48, while those for female were 0.00, 2.54, 6.29, and 14.58. The 4 knots of the consumption of milk for male were 0.00, 0.40, 2.50, and 7.00, while those for female were 0.00, 0.86, 3.50, and 7.00. We divided the male in the yogurt intake category into 3 knots (0.00, 0.58, and 7.00) because of the uneven distribution of yogurt intake. The 4 knots of the consumption of yogurt for female were 0.00, 0.23, 1.50, and 7.00. The models were adjusted for age, BMI, education level, smoking status, alcohol consumption status and physical activity, and we found that the consumption of dairy products and milk had no correlation with the risk of T2D. However, there was a linear inverse association between yogurt intake and the incidence of T2D in both male (p= 0.050) and female (p= 0.025).
RESULTS
- The association between the consumption of different types of dairy products and the risk of T2D remains controversial. This study found that consumption of dairy products was associated with a lower risk of T2D among male. In particular, the consumption of yogurt and cheese was inversely associated with the incidence of T2D in male. In female, increasing the daily consumption by 1 serving of yogurt decreased the risk of T2D by 11%.
- Our findings regarding the association between the consumption of dairy products and the risk of T2D are consistent with those of other studies [5,16,24,25]. A dose-response meta-analysis of observational studies showed similar results to those of our study. That study combined data from 22 prospective cohort studies and found that the consumption of yogurt and dairy products showed significant non-linear inverse associations with the risk of T2D, while no significant association was observed for milk [26]. A meta-analysis of 14 prospective cohort studies showed that higher yogurt intake was associated with a reduced risk of T2D [16]. In a systematic evaluation and meta-analysis, cheese and yogurt intake showed significant negative associations with the risk of T2D, while no association was found between whole milk intake and the risk of T2D [10].
- However, a recent study of 393 T2D patients from Rotterdam, the Netherlands, found no association between the consumption of dairy products and the risk of T2D [27]. Similarly, the European Prospective Investigation into Cancer and Nutrition study found no association between the total consumption of dairy products and the risk of T2D [17]. These conflicting findings may be due to differences in the definition of T2D, the geographical distribution of study populations, and the analysis methods. In the current study, the consumption of dairy products, particularly yogurt, was associated with a reduced risk of T2D in Korean adults. This finding may be related to the dairy intake pattern of Koreans. Due to lactose intolerance, many Koreans prefer to consume yogurt, which is better for intestinal health than milk [28]. There were also significantly more people who consumed at least 1 serving/day of yogurt than those who consumed at least 1 serving/day of milk. In a narrative review of the latest evidence on the benefit of consumption of dairy products for the prevention of T2D, daily intake of 3 servings of dairy products, particularly yogurt and cheese, lowered the risk of T2D [29]. A cross-sectional study on the association between dairy subgroups and prediabetes and newly diagnosed T2D among Dutch adults found a negative association between the consumption of skim and fermented dairy products and the risk of T2D [30].
- Although cheese is a fermented food like yogurt, the majority of participants in this study consumed less than 1 serving of cheese per week. This could explain the finding that cheese had a weaker effect than yogurt. Nevertheless, cheese intake was found to be beneficial for preventing T2D in male. Cheese might be a good source of vitamin K2, which is responsible for protein carboxylation by osteocalcin [10]. Osteocalcin concentration may affect insulin sensitivity and T2D by regulating the expression of insulin genes and β-cell proliferation markers [31]. In the current study, the consumption of dairy products was higher in male than in female. This could be because Korean male are more concerned about their health than Korean female [32,33].
- Certain components of dairy products, such as calcium, vitamin D, whey protein, and magnesium, have been suggested to be beneficial for T2D [34]. These components can positively affect glucose homeostasis [8]. The most active form of vitamin D is 1,25(OH)2D3 [9]. Calcium2+ signaling induced by 1,25(OH)2D3 regulates insulin secretion from pancreatic β-cells [35]. Prospective studies have reported that calcium intake lowers the prevalence of T2D [36]. Whey protein may also improve T2D, as it is composed of glycopeptides, β-lactoglobulin, α-lactalbumin, and lactoferrin, and it improves glucose clearance through differential upregulation of glucoregulatory transcripts in the liver and skeletal muscle [37]. However, in our study, those who consumed dairy products had a lower risk of T2D than those who did not consume dairy products, but the p trend values were showing no significance. This may be because the HR values had a trend of rising and falling.
- Several mechanisms could explain the negative association between yogurt intake and the risk of T2D. Obesity is one of the main causes of T2D [38]. The probiotics in yogurt reduce the risk of obesity, and this in turn may reduce the risk of T2D [11,39]. Further, yogurt intake can improve glucose homeostasis and glucose metabolism by regulating hepatic gluconeogenesis [40]. Oxidative stress plays a major role in T2D [41], and probiotics in yogurt have antioxidative mechanisms, including scavenging of reactive oxygen species, inhibiting enzymes, and lowering the activity of lactic acid bacteria [42]. The Lactobacillus fermentum ME-3 increases the total antioxidant status and decreases oxidative stress indicators [43]. Lactobacillus acidophilus and Lactobacillus have been shown to reduce oxidative stress and have anti-T2D effects [44].
- This study had some limitations. First, information on the consumption of dairy products was obtained from a self-reported quantitative questionnaire, and thus, the possibility of measurement error in the dietary assessment cannot be excluded. Second, most Korean adults consume whole milk; as such, we were unable to obtain information from the FFQ on the effect of milk by type (whole, low-fat, and skim) on the risk of T2D. Finally, the time of T2D onset could not be accurately determined due to the limited follow-up period. Although we carefully adjusted for relevant confounders, some unmeasured and residual confounders related to the consumption of dairy products and T2D may still have been presented.
- Despite these limitations, our study has many strengths. The main advantage is that, to our best knowledge, this is the first large-scale prospective cohort study to evaluate the impact of the consumption of dairy products on the risk of T2D in Korea. Given that this study considered the pattern of consumption of dairy products among Koreans, the data can be used as evidence for establishing guidelines for the consumption of dairy products in Korea. In addition, we adjusted for potential key confounders to better analyze the independent association between the consumption of dairy products and the risk of T2D. More prospective studies are required to further determine the potential benefits of consumption of dairy products in the management of T2D.
- In conclusion, the consumption of 2 or more servings of yogurt per week reduced the incidence of T2D among Korean adults compared with no or rare consumption of yogurt. In contrast, no significant association was found between the consumption of milk and the risk of T2D. Therefore, further prospective studies and clinical trials are needed to test these findings.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
-
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT) (No.2020R1C1C1014286).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Shin S. Data curation: Shin S, Zhang J. Formal analysis: Shin S, Zhang J. Funding acquisition: Shin S. Methodology: Shin S, Zhang J, Lim K. Project administration: Shin S. Visualization: Shin S, Zhang J. Writing-original draft: Zhang J. Writing- review & editing: Shin S, Zhang J, Lim K.
NOTES
ACKNOWLEDGEMENTS

| Characteristics |
Dairy product consumption (serving) |
p-value1 | |||||
|---|---|---|---|---|---|---|---|
| Non | ≤2/wk | >2-<7/wk | ≥1/day | ||||
| Male (n=16,895) | 1,700 | 5,537 | 5,746 | 3,912 | |||
| Person-years | 8,220.4 | 27,426.1 | 28,523.3 | 19,086.4 | |||
| Cases/total participants (n) | 136/1,700 | 323/5,537 | 364/5,746 | 222/3,912 | |||
| Age (yr) | 60.2±8.1 | 59.0±8.2 | 58.5±8.4 | 59.4±8.4 | <0.001 | ||
| BMI (kg/m2) | 24.2±2.8 | 24.4±2.7 | 24.3±2.7 | 24.3±2.7 | 0.047 | ||
| Educational level | <0.001 | ||||||
| Middle school or less | 503 (29.9) | 1,257 (23.0) | 1,012 (17.8) | 641 (16.6) | |||
| High school or college | 684 (40.7) | 2,248 (41.1) | 2,322 (40.8) | 1,510 (39.0) | |||
| Undergraduate school or higher | 494 (29.4) | 1,967 (36.0) | 2,356 (41.4) | 1,718 (44.4) | |||
| Smoking | <0.001 | ||||||
| Non-smokers | 409 (24.1) | 1,603 (29.0) | 1,873 (32.7) | 1,365 (35.0) | |||
| Ever smokers | 698 (41.2) | 2,290 (41.5) | 2,346 (41.0) | 1,624 (41.7) | |||
| Current smokers | 589 (34.7) | 1,629 (29.5) | 1,501 (26.2) | 909 (23.3) | |||
| Alcohol drinking | 0.007 | ||||||
| Non-drinkers | 322 (20.3) | 1,085 (20.9) | 1,117 (20.8) | 852 (23.5) | |||
| Current drinkers | 1,266 (79.7) | 4,098 (79.1) | 4,253 (79.2) | 2,779 (76.5) | |||
| Regular exercise | <0.001 | ||||||
| No | 816 (48.2) | 2,464 (44.6) | 2,235 (39.1) | 1,311 (33.6) | |||
| Yes | 878 (51.8) | 3,059 (55.4) | 3,488 (61.0) | 2,590 (66.4) | |||
| Dietary intake | |||||||
| Total energy intake (kcal/day)2 | 1,585.4±378.1 | 1,651.9±403.5 | 1,756.9±434.4 | 1,850.6±488.0 | <0.001 | ||
| Protein (g/day) | 54.8±20.5 | 56.0±19.9 | 64.6±21.9 | 72.8±25.4 | <0.001 | ||
| Protein (%) | 13.0±2.6 | 13.0±2.3 | 13.6±2.3 | 14.1±2.4 | <0.001 | ||
| Fat (g/day) | 24.1±14.5 | 25.5±13.9 | 31.9±15.3 | 37.2±17.9 | <0.001 | ||
| Fat (%) | 12.6±5.3 | 13.0±4.9 | 14.9±4.8 | 16.0±5.0 | <0.001 | ||
| Carbohydrate (g/day) | 306.3±74.8 | 313.5±72.9 | 333.2±79.2 | 354.5±87.2 | <0.001 | ||
| Carbohydrate (%) | 74.3±7.5 | 74.0±6.8 | 71.4±6.6 | 69.9±6.8 | <0.001 | ||
| Female (n=36,393) | 2,056 | 8,751 | 13,768 | 11,818 | |||
| Person-years | 9,977.1 | 43,661.2 | 69,322.1 | 59,393.6 | |||
| Cases/total participants (n) | 88/2,056 | 331/8,751 | 496/13,768 | 420/11,818 | |||
| Age (yr) | 58.7±8.0 | 57.1±7.8 | 56.8±7.5 | 57.8±7.3 | <0.001 | ||
| BMI (kg/m2) | 23.8±3.1 | 23.7±3.1 | 23.6±2.9 | 23.4±2.9 | <0.001 | ||
| Educational level | <0.001 | ||||||
| Middle school or less | 958 (47.2) | 3,359 (38.8) | 4,533 (33.3) | 3,555 (30.5) | |||
| High school or college | 811 (39.9) | 3,794 (43.8) | 6,215 (45.7) | 5,387 (46.2) | |||
| Undergraduate school or higher | 263 (12.9) | 1,507 (17.4) | 2,866 (21.1) | 2,728 (23.4) | |||
| Smoking | 0.004 | ||||||
| Non-smokers | 1,984 (96.8) | 8,472 (97.3) | 13,378 (97.7) | 11,479 (97.5) | |||
| Ever-smokers | 21 (1.0) | 71 (0.8) | 113 (0.8) | 129 (1.1) | |||
| Current smokers | 44 (2.2) | 161 (1.9) | 205 (1.5) | 160 (1.4) | |||
| Alcohol drinking | <0.001 | ||||||
| Non-drinkers | 1,495 (74.1) | 6,043 (70.4) | 8,999 (67.0) | 7,980 (68.9) | |||
| Current drinkers | 524 (26.0) | 2,538 (29.6) | 4,442 (33.1) | 3,611 (31.2) | |||
| Regular exercise | <0.001 | ||||||
| No | 1,171 (57.1) | 4,591 (52.6) | 6,433 (46.9) | 4,690 (39.8) | |||
| Yes | 881 (42.9) | 4,137 (47.4) | 7,285 (53.1) | 7,091 (60.2) | |||
| Dietary intake | |||||||
| Total energy intake (kcal/day)2 | 1,411.4±384.7 | 1,450.0±412.9 | 1,539.1±436.0 | 1,621.3±470.5 | <0.001 | ||
| Protein (g/day) | 47.2±17.2 | 49.1±18.3 | 56.2±19.8 | 65.5±23.0 | <0.001 | ||
| Protein (%) | 12.7±2.4 | 12.9±2.4 | 13.5±2.4 | 14.2±2.5 | <0.001 | ||
| Fat (g/day) | 18.1±10.7 | 20.4±12.0 | 25.9±13.3 | 32.0±15.3 | <0.001 | ||
| Fat (%) | 10.8±4.8 | 11.8±4.9 | 13.9±4.9 | 15.4±5.1 | <0.001 | ||
| Carbohydrate (g/day) | 280.0±74.4 | 285.0±78.7 | 299.5±82.9 | 322.8±88.3 | <0.001 | ||
| Carbohydrate (%) | 76.5±6.7 | 75.4±6.8 | 72.6±6.8 | 70.4±7.0 | <0.001 | ||
Values are presented as the mean±SD or as number (%); Continuous variables are reported as the mean±SD, while categorical variables are reported as number (%).
HEXA, Health Examinees; BMI, body mass index; SD, standard deviation.
1 Categorical and continuous variables were calculated using the chi-square test and general linear regression, respectively.
2 Total energy intake was adjusted using the residual method.
| Variables |
Dairy product consumption (servings) |
ptrend1 | HR for each additional serving/day | |||||
|---|---|---|---|---|---|---|---|---|
| None | ≤2/wk | >2-<7/wk | ≥1/day | |||||
| Male (n=16,895) | ||||||||
| Total dairy product consumption | ||||||||
| Cases/total participants (n) | 136/1,700 | 323/5,537 | 364/5,746 | 222/3,912 | ||||
| Person-year | 8,220.4 | 27,426.1 | 28,523.3 | 19,086.4 | ||||
| Model 1 | 1.00 (reference) | 0.66 (0.54, 0.80) | 0.70 (0.57, 0.85) | 0.65 (0.53, 0.81) | 0.101 | 0.90 (0.81, 0.99) | ||
| Model 2 | 1.00 (reference) | 0.66 (0.54, 0.82) | 0.74 (0.60, 0.90) | 0.73 (0.58, 0.91) | 0.694 | 0.94 (0.85, 1.04) | ||
| Milk consumption | ||||||||
| Cases/total participants (n) | 219/3,318 | 439/7,152 | 304/5,087 | 83/1,338 | ||||
| Person-years | 16,042.3 | 35,867.4 | 25,108.9 | 6,237.6 | ||||
| Model 1 | 1.00 | 0.81 (0.69, 0.96) | 0.82 (0.69, 0.98) | 1.05 (0.81, 1.35) | 0.709 | 1.00 (0.85, 1.18) | ||
| Model 2 | 1.00 | 0.81 (0.68, 0.95) | 0.84 (0.70, 1.00) | 1.18 (0.91, 1.54) | 0.194 | 1.06 (0.90, 1.26) | ||
| Yogurt consumption | ||||||||
| Cases/total participants (n) | 422/6,276 | 404/6,826 | 114/1,882 | 105/1,911 | ||||
| Person-years | 30,670.6 | 33,586.3 | 9,375.6 | 9,623.7 | ||||
| Model 1 | 1.00 (reference) | 0.84 (0.74, 0.97) | 0.83 (0.67, 1.02) | 0.71 (0.57, 0.88) | 0.005 | 0.82 (0.70, 0.95) | ||
| Model 2 | 1.00 (reference) | 0.85 (0.74, 0.98) | 0.90 (0.72, 1.11) | 0.75 (0.60, 0.93) | 0.035 | 0.86 (0.74, 1.01) | ||
| Non | <1/wk | ≥1/wk | ||||||
| Cheese consumption | ||||||||
| Cases/total participants (n) | 715/10,850 | 280/4,941 | 50/1,104 | |||||
| Person-year | 53,631.6 | 24,167.2 | 5,457.4 | |||||
| Model 1 | 1.00 (reference) | 0.86 (0.75, 0.99) | 0.66 (0.49, 0.88) | 0.003 | 0.37 (0.18, 0.77) | |||
| Model 2 | 1.00 (reference) | 0.89 (0.76, 1.03) | 0.69 (0.51, 0.94) | 0.016 | 0.44 (0.21, 0.94) | |||
| Female (n=36,393) | ||||||||
| Total dairy product consumption | ||||||||
| Cases/total participants (n) | 88/2,056 | 331/8,751 | 496/13,768 | 420/11,818 | ||||
| Person-years | 9,977.1 | 43,661.2 | 69,322.1 | 59,393.6 | ||||
| Model 1 | 1.00 (reference) | 0.83 (0.65, 1.04) | 0.79 (0.63, 0.99) | 0.76 (0.60, 0.96) | 0.085 | 0.91 (0.85, 0.98) | ||
| Model 2 | 1.00 (reference) | 0.85 (0.67, 1.08) | 0.87 (0.69, 1.10) | 0.88 (0.70, 1.12) | 0.987 | 0.96 (0.89, 1.03) | ||
| Milk consumption | ||||||||
| Cases/total participants (n) | 201/5,277 | 495/13,011 | 489/13,900 | 150/4,205 | ||||
| Person-years | 25,722.4 | 66,000.1 | 69,972.6 | 20658.9 | ||||
| Model 1 | 1.00 (reference) | 0.91 (0.77, 1.08) | 0.87 (0.74, 1.03) | 0.92 (0.74, 1.13) | 0.387 | 0.95 (0.84, 1.09) | ||
| Model 2 | 1.00 (reference) | 0.93 (0.78, 1.09) | 0.91 (0.77, 1.08) | 1.01 (0.81, 1.25) | 0.871 | 1.02 (0.90, 1.17) | ||
| Yogurt consumption | ||||||||
| Cases/total participants (n) | 415/10,564 | 549/15,143 | 183/5,344 | 188/5,342 | ||||
| Person-years | 51,965.4 | 75,878.0 | 27,352.3 | 27158.3 | ||||
| Model 1 | 1.00 (reference) | 0.91 (0.80, 1.04) | 0.79 (0.67, 0.94) | 0.81 (0.68, 0.96) | 0.008 | 0.85 (0.76, 0.95) | ||
| Model 2 | 1.00 (reference) | 0.94 (0.83, 1.08) | 0.88 (0.74, 1.05) | 0.87 (0.73, 1.04) | 0.115 | 0.89 (0.79, 0.99) | ||
| Non | <1/wk | ≥1/wk | ||||||
| Cheese consumption | ||||||||
| Cases/total participants (n) | 787/19,305 | 397/12,182 | 151/4,906 | |||||
| Person-years | 97,340.2 | 60,771.0 | 24,242.8 | |||||
| Model 1 | 1.00 (reference) | 0.88 (0.78, 0.99) | 0.84 (0.70, 1.00) | 0.064 | 0.85 (0.61, 1.18) | |||
| Model 2 | 1.00 (reference) | 0.94 (0.83, 1.07) | 0.96 (0.80, 1.15) | 0.584 | 1.03 (0.75, 1.43) | |||
Model 1 is adjusted for age (continuous); Model 2 is adjusted for age (continuous), body mass index (continuous), educational level (≤middle school, high school or college, ≥undergraduate school), smoking status (never, ever, current, unknown), alcohol drinking status (never, ever, unknown), physical activity (yes, no, unknown), and total intake (continuous).
HR, lhazard ratio; CI, confidence interval; HEXA, Health Examinees.
1 Calculated by categories of milk consumption; Associations were tested using the median values for each category and were treated as continuous variables.
- 1. Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019;157:107843.ArticlePubMed
- 2. IDF Diabetes Atlas. Diabetes around the world in 2021 [cited 2021 Apr 16]. Available from: https://diabetesatlas.org/.
- 3. Shim HT. 1 in 7 Korean adults has diabetes; cure rate remains low; 2020 [cited 2021 Apr 16]. Available from: http://www.koreabiomed.com/news/articleView.html?idxno=9508.
- 4. Wu Y, Ding Y, Tanaka Y, Zhang W. Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. Int J Med Sci 2014;11:1185-1200.ArticlePubMedPMC
- 5. Díaz-López A, Bulló M, Martínez-González MA, Corella D, Estruch R, Fitó M, et al. Dairy product consumption and risk of type 2 diabetes in an elderly Spanish Mediterranean population at high cardiovascular risk. Eur J Nutr 2016;55:349-360.ArticlePubMedPDF
- 6. Pereira PC. Milk nutritional composition and its role in human health. Nutrition 2014;30:619-627.ArticlePubMed
- 7. Melnik BC. Milk--the promoter of chronic Western diseases. Med Hypotheses 2009;72:631-639.ArticlePubMed
- 8. Tremblay A, Gilbert JA. Milk products, insulin resistance syndrome and type 2 diabetes. J Am Coll Nutr 2009;28 Suppl 1:91S-102S.ArticlePubMed
- 9. Christakos S, Hewison M, Gardner DG, Wagner CL, Sergeev IN, Rutten E, et al. Vitamin D: beyond bone. Ann N Y Acad Sci 2013;1287:45-58.ArticlePubMedPMCPDF
- 10. Gao D, Ning N, Wang C, Wang Y, Li Q, Meng Z, et al. Dairy products consumption and risk of type 2 diabetes: systematic review and dose-response meta-analysis. PLoS One 2013;8:e73965.ArticlePubMedPMC
- 11. Astrup A. Yogurt and dairy product consumption to prevent cardiometabolic diseases: epidemiologic and experimental studies. Am J Clin Nutr 2014;99(5 Suppl):1235S-1242S.ArticlePubMed
- 12. Kim D, Kim J. Dairy consumption is associated with a lower incidence of the metabolic syndrome in middle-aged and older Korean adults: the Korean Genome and Epidemiology Study (KoGES). Br J Nutr 2017;117:148-160.ArticlePubMed
- 13. Park SJ, Park J, Song HJ, Lee CH, Lee HJ. Association between dairy product intake and hypertriglyceridemia in Korean adults. Nutr Res Pract 2020;14:152-159.ArticlePubMedPMCPDF
- 14. Beydoun MA, Fanelli-Kuczmarski MT, Beydoun HA, Dore GA, Canas JA, Evans MK, et al. Dairy product consumption and its association with metabolic disturbance in a prospective study of urban adults. Br J Nutr 2018;119:706-719.ArticlePubMedPMC
- 15. Talaei M, Pan A, Yuan JM, Koh WP. Dairy intake and risk of type 2 diabetes. Clin Nutr 2018;37:712-718.ArticlePubMedPMC
- 16. Chen M, Sun Q, Giovannucci E, Mozaffarian D, Manson JE, Willett WC, et al. Dairy consumption and risk of type 2 diabetes: 3 cohorts of US adults and an updated meta-analysis. BMC Med 2014;12:215.ArticlePubMedPMCPDF
- 17. Sluijs I, Forouhi NG, Beulens JW, van der Schouw YT, Agnoli C, Arriola L, et al. The amount and type of dairy product intake and incident type 2 diabetes: results from the EPIC-InterAct Study. Am J Clin Nutr 2012;96:382-390.ArticlePubMed
- 18. Kim J, Hwang JY, Kim KN, Choi YJ, Chang N, Huh KB. Relationship between milk and calcium intake and lipid metabolism in female patients with type 2 diabetes. Yonsei Med J 2013;54:626-636.ArticlePubMedPMC
- 19. Jeon J, Jang J, Park K. Effects of consuming calcium-rich foods on the incidence of type 2 diabetes mellitus. Nutrients 2018;11:31.ArticlePubMedPMC
- 20. United States Department of Agriculture. Dairy: world markets and trade [cited 2021 May 19]. Available from: https://apps.fas.usda.gov/psdonline/app/index.html#/app/downloads.
- 21. Health Examinees Study Group. The Health Examinees (HEXA) study: rationale, study design and baseline characteristics. Asian Pac J Cancer Prev 2015;16:1591-1597.ArticlePubMed
- 22. Ahn Y, Kwon E, Shim JE, Park MK, Joo Y, Kimm K, et al. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr 2007;61:1435-1441.ArticlePubMedPDF
- 23. Korean Diabetes Association. 2015 Treatment guidelines for diabetes (5th edition). [cited 2021 May 19]. Available from: https://www.diabetes.or.kr/bbs/index.html?code=e_resource2.
- 24. Hruby A, Ma J, Rogers G, Meigs JB, Jacques PF. Associations of dairy intake with Incident prediabetes or diabetes in middle-aged adults vary by both dairy type and glycemic status. J Nutr 2017;147:1764-1775.ArticlePubMedPMC
- 25. Fan M, Li Y, Wang C, Mao Z, Zhang L, Yang X, et al. Consumption of dairy products in relation to type 2 diabetes mellitus in Chinese people: the Henan Rural Cohort study and an updated meta-analysis. Nutrients 2020;12:3827.ArticlePubMedPMC
- 26. Gijsbers L, Ding EL, Malik VS, de Goede J, Geleijnse JM, Soedamah-Muthu SS. Consumption of dairy foods and diabetes incidence: a dose-response meta-analysis of observational studies. Am J Clin Nutr 2016;103:1111-1124.ArticlePubMed
- 27. Brouwer-Brolsma EM, van Woudenbergh GJ, Oude Elferink SJ, Singh-Povel CM, Hofman A, Dehghan A, et al. Intake of different types of dairy and its prospective association with risk of type 2 diabetes: the Rotterdam Study. Nutr Metab Cardiovasc Dis 2016;26:987-995.ArticlePubMed
- 28. Jackson KA, Savaiano DA. Lactose maldigestion, calcium intake and osteoporosis in African-, Asian-, and Hispanic-Americans. J Am Coll Nutr 2001;20(2 Suppl):198S-207S.ArticlePubMed
- 29. Mitri J, Mohd Yusof BN, Maryniuk M, Schrager C, Hamdy O, Salsberg V. Dairy intake and type 2 diabetes risk factors: a narrative review. Diabetes Metab Syndr 2019;13:2879-2887.ArticlePubMed
- 30. Brouwer-Brolsma EM, Sluik D, Singh-Povel CM, Feskens EJ. Dairy product consumption is associated with pre-diabetes and newly diagnosed type 2 diabetes in the Lifelines Cohort Study. Br J Nutr 2018;119:442-455.ArticlePubMed
- 31. Beulens JW, van der A DL, Grobbee DE, Sluijs I, Spijkerman AM, van der Schouw YT. Dietary phylloquinone and menaquinones intakes and risk of type 2 diabetes. Diabetes Care 2010;33:1699-1705.ArticlePubMedPMCPDF
- 32. Woo D, Lee Y, Park S. Associations among working hours, sleep duration, self-rated health, and health-related quality of life in Korean men. Health Qual Life Outcomes 2020;18:287.ArticlePubMedPMCPDF
- 33. Lee SY, Kim SJ, Yoo KB, Lee SG, Park EC. Gender gap in self-rated health in South Korea compared with the United States. Int J Clin Health Psychol 2016;16:11-20.ArticlePubMedPMC
- 34. Mozaffarian D, Wu JH. Flavonoids, dairy foods, and cardiovascular and metabolic health: a review of emerging biologic pathways. Circ Res 2018;122:369-384.ArticlePubMedPMC
- 35. Ahn C, Kang JH, Jeung EB. Calcium homeostasis in diabetes mellitus. J Vet Sci 2017;18:261-266.ArticlePubMedPMCPDF
- 36. Pittas AG, Dawson-Hughes B, Li T, Van Dam RM, Willett WC, Manson JE, et al. Vitamin D and calcium intake in relation to type 2 diabetes in women. Diabetes Care 2006;29:650-656.ArticlePubMedPDF
- 37. Zapata RC, Singh A, Pezeshki A, Nibber T, Chelikani PK. Whey protein components - lactalbumin and lactoferrin - improve energy balance and metabolism. Sci Rep 2017;7:9917.ArticlePubMedPMCPDF
- 38. Apovian CM, Okemah J, O’Neil PM. Body weight considerations in the management of type 2 diabetes. Adv Ther 2019;36:44-58.ArticlePubMedPMCPDF
- 39. Salas-Salvadó J, Guasch-Ferré M, Díaz-López A, Babio N. Yogurt and diabetes: overview of recent observational studies. J Nutr 2017;147:1452S-1461S.ArticlePubMed
- 40. Veldhorst M, Smeets A, Soenen S, Hochstenbach-Waelen A, Hursel R, Diepvens K, et al. Protein-induced satiety: effects and mechanisms of different proteins. Physiol Behav 2008;94:300-307.ArticlePubMed
- 41. Stephens JW, Khanolkar MP, Bain SC. The biological relevance and measurement of plasma markers of oxidative stress in diabetes and cardiovascular disease. Atherosclerosis 2009;202:321-329.ArticlePubMed
- 42. Lin MY, Yen CL. Antioxidative ability of lactic acid bacteria. J Agric Food Chem 1999;47:1460-1466.ArticlePubMed
- 43. Songisepp E, Kals J, Kullisaar T, Mändar R, Hütt P, Zilmer M, et al. Evaluation of the functional efficacy of an antioxidative probiotic in healthy volunteers. Nutr J 2005;4:22.ArticlePubMedPMCPDF
- 44. Yadav H, Jain S, Sinha PR. Antidiabetic effect of probiotic dahi containing Lactobacillus acidophilus and Lactobacillus casei in high fructose fed rats. Nutrition 2007;23:62-68.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
- Usual intake of dairy products and the chance of pre-diabetes regression to normal glycemia or progression to type 2 diabetes: a 9-year follow-up
Zahra Bahadoran, Parvin Mirmiran, Fereidoun Azizi
Nutrition & Diabetes.2024;[Epub] CrossRef - Cheese consumption and multiple health outcomes: an umbrella review and updated meta-analysis of prospective studies
Mingjie Zhang, Xiaocong Dong, Zihui Huang, Xue Li, Yue Zhao, Yingyao Wang, Huilian Zhu, Aiping Fang, Edward L. Giovannucci
Advances in Nutrition.2023; 14(5): 1170. CrossRef - Effect of Milk and Cultured Milk Products on Type 2 Diabetes: A Global Systematic Review and Meta-analysis of Prospective Cohort Studies
Viswanathan Mohan, Kuzhandhaivelu Abirami, Valangaiman Sriram Manasa, Anandakumar Amutha, Balaji Bhavadharini, Rinky Rajput, Nagarajan Lakshmipriya, Chowdary Sruthi, Ranjit Mohan Anjana, Ranjit Unnikrishnan, Vasudevan Sudha, Kamala Krishnaswamy
Journal of the Indian Institute of Science.2023; 103(1): 167. CrossRef - Probiotic potential of fermented foods and their role in non-communicable diseases management: An understanding through recent clinical evidences
A. Nithya, Sourav Misra, Chirasmita Panigrahi, Chandrakant Genu Dalbhagat, Hari Niwas Mishra
Food Chemistry Advances.2023; 3: 100381. CrossRef - Dairy intake and risk of type 2 diabetes: results of a large prospective cohort
Shunming Zhang, Ge Meng, Qing Zhang, Li Liu, Hongmei Wu, Yeqing Gu, Xuena Wang, Juanjuan Zhang, Shaomei Sun, Xing Wang, Ming Zhou, Qiyu Jia, Kun Song, Yan Borné, Emily Sonestedt, Le Ma, Lu Qi, Kaijun Niu
Food & Function.2023; 14(21): 9695. CrossRef - Association of milk consumption with management and incidence of hypertension among South Korean adults: A prospective analysis of the health examinees study cohort
Hyein Jung, Geongu Lee, Kyungjoon Lim, Sangah Shin
Nutrition, Metabolism and Cardiovascular Diseases.2022; 32(11): 2515. CrossRef - Association between dairy consumption and the risk of diabetes: A prospective cohort study from the China Health and Nutrition Survey
Yucheng Yang, Xiaona Na, Yuandi Xi, Menglu Xi, Haibing Yang, Zhihui Li, Ai Zhao
Frontiers in Nutrition.2022;[Epub] CrossRef - Association of dairy consumption patterns with the incidence of type 2 diabetes: Findings from Alberta's Tomorrow Project
Emad Yuzbashian, Mohammadreza Pakseresht, Jennifer Vena, Catherine B. Chan
Nutrition, Metabolism and Cardiovascular Diseases.2022; 32(12): 2760. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite