Abstract
-
OBJECTIVES
- Vaccinations for infectious diseases are opposed despite their achievement, and this opposition has recently been revealed in Korea. However, research in Korea has not been vigorous. The authors studied why some Korean parents hesitate to vaccinate their children by applying the health belief model.
-
METHODS
- Parents who hesitate to vaccinate and parents who do not were surveyed in alternative education preschools and elementary schools. They were classified into four types of hesitancy and statistically compared.
-
RESULTS
- Among the 129 subjects, 43 vaccinated without hesitancy, 20 vaccinated on time with hesitancy, 32 vaccinated with a deliberate delay of one month or longer, and 34 did not vaccinate. Vaccination increased with an increase in the awareness that severe outcomes can occur when unvaccinated. Concerns about adverse reactions from vaccinations or direct/indirect experiences affected refusal. Furthermore, perceptions of the lack of meaningfulness of vaccinations, distrust of policy and safety management, influence of leaders or activists in joined organizations, and experts of Korean traditional or alternative medicine affected refusal. Explanations by doctors, text messages and mails from institutions, and concerns about disadvantages caused by not complying with government policies increased vaccination.
-
CONCLUSIONS
- The reasons for vaccine hesitancy and acceptance were similar to the results of international research. Health authorities and professionals should communicate sufficiently and appropriately with hesitant parents and find ways to rationally resolve social conflicts. However, this sample was small and there is little Korean research, so more in-depth and diverse researchs are needed.
-
Keywords: Vaccine hesitancy, Vaccination refusal, Health belief model, Korea
INTRODUCTION
- Vaccination against infectious diseases is a modern scientific achievement, and it is recognized as an essential protector for the lives and health of children [1]. However, there has been continuous trends of vaccination refusal in many countries to date from the first smallpox vaccination in the eighteenth century [2,3]. In particular, there are still many anti-vaccination groups in advanced countries, such as the USA, Europe, Australia, and Japan, even though the socioeconomic barriers have been sufficiently eliminated [1,4-6]. Furthermore, researchs on the characteristics of the groups, the socioeconomic effects, mandatory or liberalization policies, and ethics are ongoing [4,5,7-10].
- Existing studies often apply the concept of vaccine hesitancy (VH) presented by the World Health Organization (WHO) in regard to parental attitudes and decisions about required child vaccinations. This refers to deliberately delaying or refusing vaccination even though services are accessable [7]. Based on this, many studies make four classifications: First, vaccination without hesitancy; second, vaccination on time with hesitancy; third, deliberately delaying vaccination for one month or longer with hesitancy; and fourth, deliberate vaccination refusal with hesitancy [11,12].
- The proportion of required child vaccinations is known to be high in Korea, and VH studies are rarely reported [13,14]. The concept and classifications of VH are also unfamiliar in Korea. However, with “ANAKI” (Korean abbreviation of “raising children without medication”) becoming a societal issue in 2017, movements to refuse modern medicine including vaccines have appeared. Similar to there being parents who hestiate vaccinations or medical treatments in alternative education preschools and schools overseas [15], authors knew that those parents also existed in Korean alternative education facilities. Of course, their scale needs to be identified through a national survey, but there are practical limitations. Therefore, authors first surveyed accessible parents to examine their VH reasons based on the Health Belief Model (HBM).
MATERIALS AND METHODS
- The subjects were recruited from alternative education preschools and elementary schools in which there would presumedly be VH parents. There are 78 locations in the Association of Alternative Education Preschools, among which 26 locations are in Southern Gyeonggi province and 9 are in Northern. Preschools outside association could not be identified. Although 246 locations (59 in Gyeonggi) of alternative education schools are registered in their Association, most are middle or high schools. As there are no elementary school dataset, it was estimated 20 locations by checking website one by one. It was difficult to get a standardized sample. The area in which many are located and which authors could directly visit was Southern Gyeonggi. Twenty-six preschools and 7 elementary schools were contacted in person, by mail, by phone, and by e-mail. The subject selection criteria at the participating facilities were Korean parents with one child or more in second grade in elementary school or younger as of 2018 (i.e., a child born after January 1, 2010). According to the standard schedule of the Korea Centers for Disease Control and Prevention, child vaccinations are completed at the age of 12. Therefore, they were first targeted. However, considering the repeated revision of schedule, only 2 additional vaccinations between the ages of 10 and 12, decreased parental vaccination interest after the child starts elementary school, and the difficulty to remember previous vaccinations, the birth year were limited to 2010 or later. Also, underaged parents, non-Korean or naturalized parents, and caregivers of grandchildren were excluded.
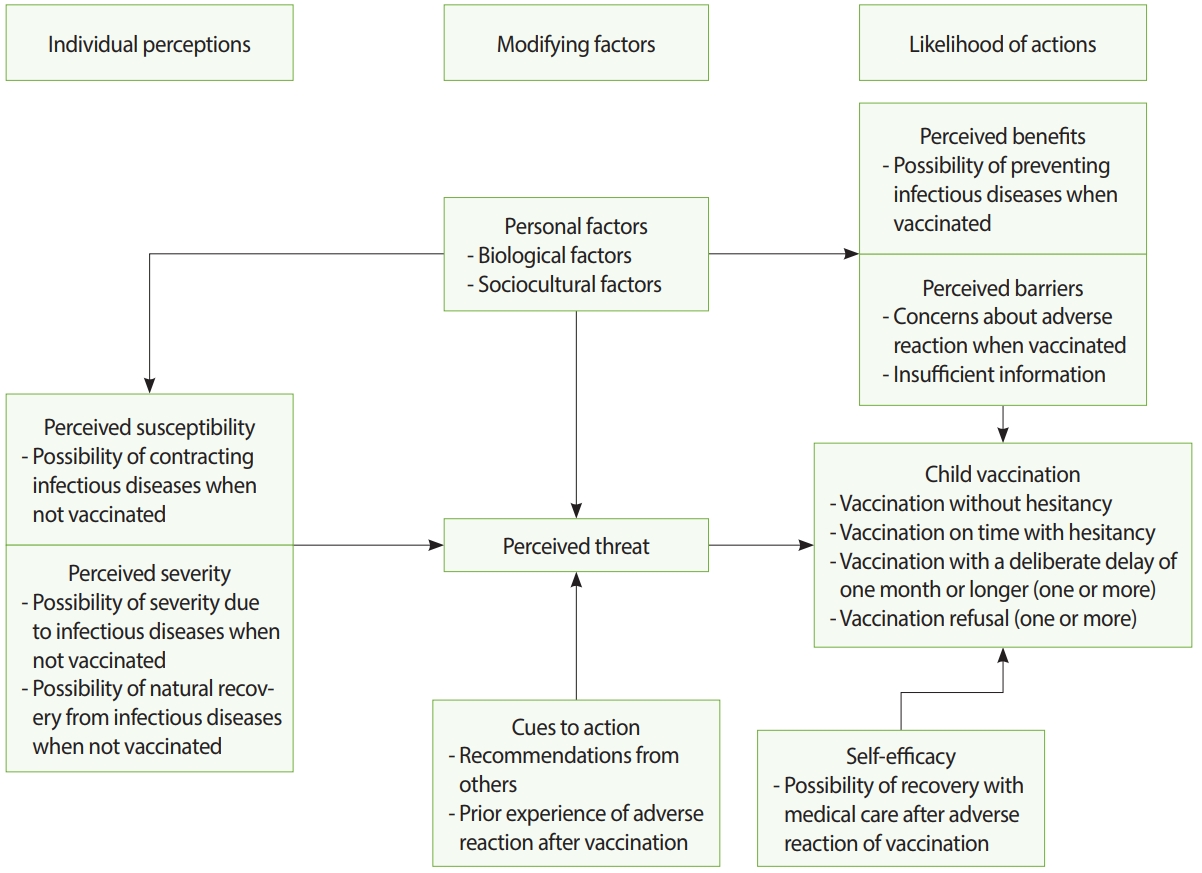
- The authors applied a structured qustionnaire that was revised based on previous studies. The qustionnaire was comprised of basic human information, common HBM questions, and items relating to the four VH classifications. The HBM questions were structured by referencing the previous studies and covered the following topics: perceived susceptibility and severity, which are individual perceptions; personal factors and cues to action, which are modifying factors; and perceived benefits and barriers, which refer to the possibility of behavior [5,11,16,17]. Previous questions included both interrogative and descriptive sentences, and there were cases of pinpointing a specific vaccination and cases of not. The authors designed the items to be as descriptive as possible so that the subjects could respond whether they agreed or not. The Korean vaccination schedule was presented and the responses to overall vaccination were requested. Additionally, including self-efficacy questions which has been included in the HBM in recent studies [16], the model determining the four VH types were structuralized (Figure 1). Each items reflected VH using the agreement of the responses. Meanwhile, specific questions of the reason for vaccination or hesitation were structured with references [6,18-20]. Items asked the reason for hesitating, delaying, or refusing vaccination; the person who made impacts; and the reason for ultimately vaccinating. Items that fit Korean characteristics, such as Korean traditional medicine, disadvantages due to non-cooperation with government policies, and text messages from institutions, were added. The Korean version questionnaire is attached (Supplementary Material 1). The questionnaires were directly distributed at the facilities, delivered through representatives or teachers, and mailed.
- Each participant was given one tricolored pen without other compensation. Statistical analyses were performed using SPSS version 23 (IBM Co., Armonk, NY, USA). The chi-square test for trend test was done to compare groups, and analysis of variance was performed on continuous variables. Additionally, logistic regression analysis was done with HBM factors. The multicollinearity among the variables was identified with the Cramer’s V value. The significance level was 0.05.
- Ethics statement
- This study was approved by the Institutional Review Board of Ajou University Hospital on July 24, 2018. The approved informed consent and questionnaire were used.
RESULTS
- Surveys were conducted in 12 preschools and 2 elementary schools between August and November 2018. A total of 141 subjects participated, with 1 to 33 subjects per location. Among those, 1 without children born in 2010 or later, 6 with children with medical illnesses that make vaccinations impossible, 5 with no responses, and 3 with no response on whether the child lives together were excluded. After excluding 12 subjects including duplicates, 129 subjects were finally analyzed.
- They were comprised of 43 who vaccinated without hesitancy, 20 who vaccinated on time with hesitancy, 32 who delayed vaccination for one month or longer, and 34 who refused vaccination. There were 119 women whose mean age was 38.1 years old (28-46 years old), among whom 125 were married and 127 lived in Gyeonggi. As for education level, there were 3 high school graduates, 96 college/university graduates, and 31 graduate school graduates. The subjective income levels were upper class for 3 subjects, middle class for 109 subjects, lower class for 14 subjects, and 3 did not respond. The number of children was 1 for 47 subjects, 2 for 69 subjects, and 3 for 13 subjects. The differences among the four groups by item showed no significant results in all items except income level; the vaccination refusal group had more “lower-level” income than the other groups at 23.5% (p=0.006) (Table 1).
- Questions on whether the subject saw the danger of infectious diseases and the benefits of vaccination as important were about perceived susceptibility, the first item on perceived severity, the perceived benefits, and self-efficacy. For all four, positive responses were higher with less VH and this trend was statistically significant. The questions about negative disposition toward vaccinations - the first item on perceived barriers, the second item on cues to action, and the second item on perceived severity - showed increasing statistical tendencies for negativity toward vaccinations as the classification became closer to vaccination refusal. Although the second item on perceived barriers and first and third items on cues to action had statistical tendencies, the number of respondents was somewhat lower for the refusal group compared to the deliberately delay group (Table 2).
- To identify the correlations among the 10 HBM variables and subjective income levels, which showed statistical differences, Cramer’s V values were calculated. As a result, pairs that exceed 0.5 were perceived susceptibility and the first item of perceived severity (0.595) and perceived susceptibility and perceived benefits (0.579). Pairs that exceed 0.4 were the first item of perceived severity and perceived benefits (0.480) and the first and third items of cues to action (0.411). Cramer’s V values between the other variables were all below 0.4.
- A logistic regression analysis using nine HBM items was computed after excluding the perceived susceptibility item based on Cramer’s V value of 0.5. Income levels, which was significant among the socio-demographic variables, was excluded because of large differences in the numbers of subjects in the 3 groups: 3 upper-level, 109 middle-level, and 14 lower-level. For the binary logistic regression, vaccination was recategorized by combining vaccination without hesitancy and vaccination on time with hesitancy and by combining delay and refusal. The chi-square analyses after the combinations still showed significance levels below 0.05. The odds ratios before the adjustment were statistically significant for all items. After the adjustment, the perceived severity was significant (p=0.042) (Table 3).
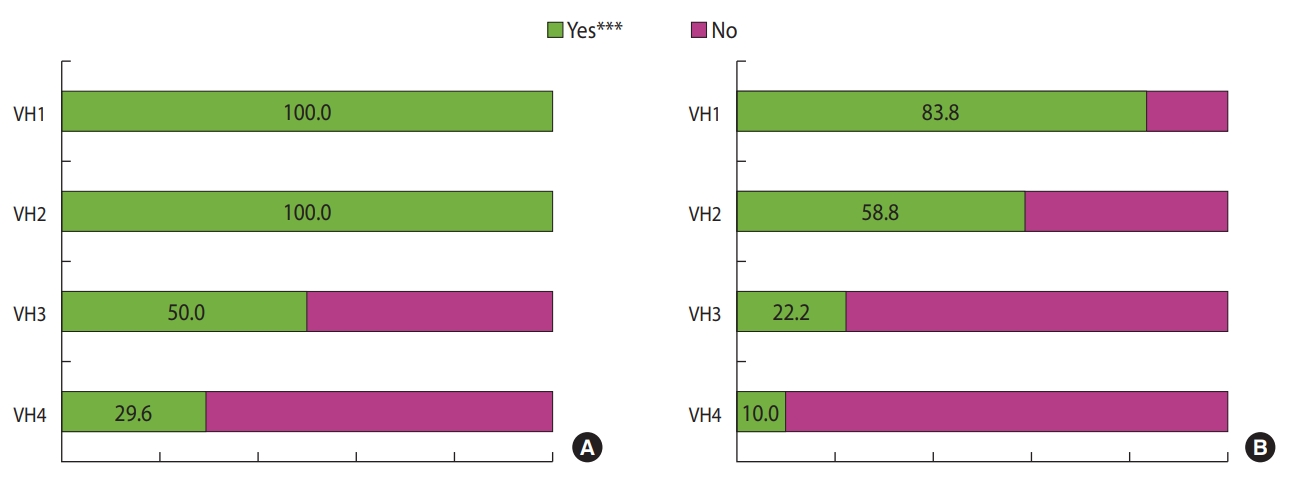
- Apart from HBM questions, all four groups were asked about the perception of the necessity and safety of vaccinations. The result showed statistical tendencies of lower VH being associated with a higher level of perception of necessity (p<0.001) and safety (p<0.001) (Table 2). Sixty-six subjects stated that they refused or deliberately delayed vaccination for one month or longer. After allowing multiple responses, delayed or refused vaccines for Japanese encephalitis were the most common at 41 cases, followed by 34 cases of diphtheria, tetanus toxoid, acellular pertussis (DTaP), 34 cases of measles, mumps, rubella (MMR), 32 cases of inactivated polio vaccine (IPV), 27 cases of chickenpox vaccine, 15 cases of Bacillus Calmette-Guérin (BCG), and 15 cases of hepatitis B vaccine. There were 20 cases of non-vaccination despite not knowing which one.
- The hesitant reasons were asked from the group who vaccinated on time with hesitancy, the delay group, and the refusal group. Concerns and experiences of adverse reactions with vaccinations were 60% or more in all groups. The percentage that they distrusted vaccination safety management was around or above 50% as well. The most common reasons for hesitancy by group were as follows: For the group who vaccinated on time with hesitancy, the reasons were in the order of concerns and experiences of adverse reactions, distrust of safety management, and distrust of government policies. For the delay group, the reasons were in the order of concerns and experiences of adverse reactions, distrust of government policies, and distrust of safety management. For the refusal group, the reasons were in the order of concerns and experiences of adverse reactions, distrust of safety management, and the meaninglessness of vaccinations (Table 4). The persons who affected the hesitancy were as follows: For the group who vaccinated on time with hesitancy, the order was online anti-vaccination activists, decision by oneself, and acquaintances. For the delay group, the order was decision by oneself, anti-vaccination activists, acquaintances, and family. For the refusal group, the order was decision by oneself, anti-vaccination activists, acquaintances, activists in joined organizations, and experts of Korean traditional or alternative medicine (Table 5).
- The reasons of vaccine acceptance were asked from the group who vaccinated without hesitancy, the group who vaccinated on time with hesitancy, and the group who deliberately delayed vaccination. For the no hesitant group, the reasons were in the order of decision by the parents themselves (72.1%), text messages or mails from medical/health facilities (53.5%), and the explanation of doctors who saw their children (48.8%). For the on-time vaccination group with hesitancy, the reasons were in the order of decision by the parents (85.0%) and concerns about the disadvantages to the children upon failure to cooperate with government policies (30.0%). For the delay group, the reasons were in the order of decision by the parents (59.4%), concerns about the disadvantages (37.5%), and text messages or mails from facilities (28.1%).
DISCUSSION
- Previous studies [11,21,22] reported that the hesitant groups tends to have higher education and income levels. In this study, the proportions of college/university graduation or higher were high at 96.9% and 100.0% for the delay group and refusal group, respectively. However, the proportions were also high at 97.7% and 95.0% for the no hesitant group and the on-time vaccination group with hesitancy, respectively, showing no differences between the groups. Income level was measured via subjective responses rather than quantitative measurements. Although the response for “middle-level” was high for the no hesitant group, the vaccination group with hesitancy, and the delay group at 85.7%, 95.0%, 93.8%, and 79.4% of the refusal group was “middle” and 23.5% was “low,” showing statistical differences. However, only the tendency could be examined because of small sample size, and the reason could not be identified.
- The analysis with the HBM showed that the group with lower VH had more concerns about infectious diseases when not vaccinated, which affected the perceived threat and led to vaccination acceptance. In contrast, the more hesitant group thought highly of the possibility of natural recovery even when exposed to infections, which lowered the perceived threat and led to vaccination refusal. Furthermore, lower hesitancy was associated with the perception of benefits that vaccination can prevent infections, having a positive effect to accept vaccination. In contrast, concerns about the adverse reactions from vaccination or not being provided with sufficient information about vaccination appeared to be higher in the hesitant groups and affected refusal. However, insufficient information exceeded 50% in the vaccination groups as well. Cues to action were direct/indirect experiences of adverse reactions. If the level of this factor increased, the perceived threat decreased and affected refusal. For all three relevant items, it was shown that the more hesitant groups had a higher level of this factor and this affected refusal. The self-efficacy item, which was the belief that recovery can sufficiently be made from adverse reactions through medical treatment, was higher in level for groups closer to vaccination without hesitancy; thus, it had a positive impact on vaccination. All factors showed statistical significance in the univariate analyses (Table 2), so the HBM-VH decision model was valid. The multivariate analysis chose a logistic regression rather than combined analyses, such as a structural equation model, considering the small sample size. As a result, the perception that the child could experience infections leading to severe conditions when not vaccinated, which was an item of perceived severity, was significant to accept vaccines (Table 3). To identify the reason for the group differences in the perception of this factor, a large-sample between-group comparison study or qualitative research on the refusal group is necessary.
- Delayed or refused Japanese encephalitis vaccine, DTaP, MMR, and IPV were slightly more common. The first dose of DTaP and IPV start two months after birth, there are a number of doses until the age of four to six. The first dose of Japanese encephalitis vaccine and MMR come after 12 months. In contrast, the number of refusals for BCG and hepatitis B, which are vaccinated immediately after birth, was relatively low. These orders are assumed to be given because personal experiences with adverse reactions affected future vaccination refusal. Similar items of HBM were significant as well. Additionally, for all three groups of vaccination with hesitancy, delay, and refusal, the concerns and experiences of adverse reactions were the greatest reason for hesitation at 65.0-75.8% (Table 4), trust in the safety decreased (Figure 2), and more than half of all four VH groups responded that the vaccination information was insufficient. These results showed the importance of advertisement and communication. Additionally, when considering the distrust in the vaccination safety management and government policies (Table 4), understanding of the vaccination policies and management systems along with information about adverse reactions is important for communication. Being provided with sufficient information and communicating with experts are the rights of the parents who decide vaccination and are important factors. There are various overseas studies on which approach is effective, and the results varied due to the differences in the social systems and cultures of each country [5,8,10]. Korean research is needed to identify suitable approachs.
- As for reasons to hesitate and refuse vaccination, the concerns and experiences of adverse reactions, distrust of policies and safety management, and not recognizing the meaningfulness of the infection prevention were the main reasons (Table 4). It can be hypothesized that the hesitant groups do not sufficiently trust the healthcare system. Furthermore, persons who affected vaccination refusal were online anti-vaccination activists, personnel of civil society groups, and experts of Korean traditional or alternative medicine. In particular, the impact of these people appeared greater for the refusal group. The effect of alternative medicine was reported in overseas studies as well [21]. However, distinguishment of Korean traditional medicine and alternative medicine is a task for the future studies because Korean official system includes traditional medicine. Additionally, the impact of online anti-vaccination activists was identified, similar to the previous studies [3,6,22]. To appropriately respond to the VH issue, health authorities and professionals must recognize these social movements and the impact of related persons [2]. Meanwhile, it must also be considered that criticism, regulation, and punishment-centered approaches and seeing citizens as the passive subjects of education/advertisement are ineffective in democratic countries [22-24]. Combining all of these facets, healthcare professionals must sufficiently and appropriately communicate with people who affect VH and affected parents [11,24-26].
- The factors that led to ultimately accepting vaccination were doctors’ explanation, disadvantages to the unvaccinated child, and text messages and mails from institutions. Although overseas studies showed similar results that doctors are the most decisive [11,12], the contributed proportion of doctors did not exceed 30% in the group that vaccinated with hesitancy in this study. It is necessary to research the impact of the Korean clinical environment, with its short doctor consultations. In previous studies, general physicians played important roles in countries with strong primary healthcare and delivery systems, whereas pediatricians played important roles in countries that directly accessed pediatricians as primary caregivers [3,27]. The status and future plans of Korea should be studied considering them. Meanwhile, the proportion that decides to vaccinate due to concerns about the disadvantages faced by unvaccinated children is also high. There are researchs that regulation can have positive or negative effects on the rate of vaccination [12,28,29]. In particular, there is a tendency for the strengthening of regulations to have a negative effect in countries with stronger sovereignty of the people and a more stable democratic system [9,10,30]. Korean research that considers the historical, social, and cultural backgrounds is necessary [31].
- Generally, the aim of VH research is to examine how to get parents to accept vaccines [1,5,7,22]. This is because if the hesitant population is large enough, there can be a ripple effect on the infection spread [30,32]. However, because Korea estimates that they are very small in number, it is not easy to make a significant ripple effects [13,14]. Also, heavy-handed regulation can increase the conflicts and avoidance rather than resolution [3,12,22,33]. Moreover, considering the research results that they have low trust in the healthcare system, caution must be taken in instituting regulation-based policies [34]. A resolution in which social agreement is possible must be found through comprehensive trust-building communication with VH parents [2,35].
- VH researchs to date has mainly focused on Western countries and Japan, and status investigations or research in Korea have been insufficient. This research has limited representativeness because it was not a national survey and was conducted on a small number of parents in specific groups. However, this study can be a reference for large-scale or qualitative studies in the future, because this was conducted in alternative education facilities, in which VH parents are possibly concentrated. Particularly, the limitations in the representativeness and sample size was complmented by the HBM that examined how the positive and negative reasons for vaccination link to whether one vaccinates. The result found that VH factors are making impacts, similar to previous studies conducted in foreign countries. If status investigations show that there are hesitant peoples of considerable size with the possibility of expansion, like in other developed countries, this study can be an important reference for future studies and policy making. Meanwhile, Korea has characteristics such as official system for traditional medicine, an incomplete primary healthcare system and short consultations, and disadvantages about unvaccinated children. Future researchs are particularly important focusing on the Korea-specific situations.
SUPPLEMENTARY MATERIALS
NOTES
-
The authors have no conflicts of interest to declare for this study.
-
AUTHOR CONTRIBUTIONS
Conceptualization: SYL, KC. Data curation: KC, SYL. Formal analysis: KC, SYL. Funding acquisition: None. Methodology: SYL, KC. Project administration: KC. Visualization: KC, SYL. Writing – original draft: KC, SYL. Writing – review & editing: SYL, KC.
ACKNOWLEDGEMENTS
We express deep gratitude to Advisory Professor Jakyoung Lee of Ajou University Graduate School of Public Health, who provided help with structuring the questionnaire items by reflecting the HBM.
Figure 1.Process of child vaccination decision making according to the Health Belief Model.
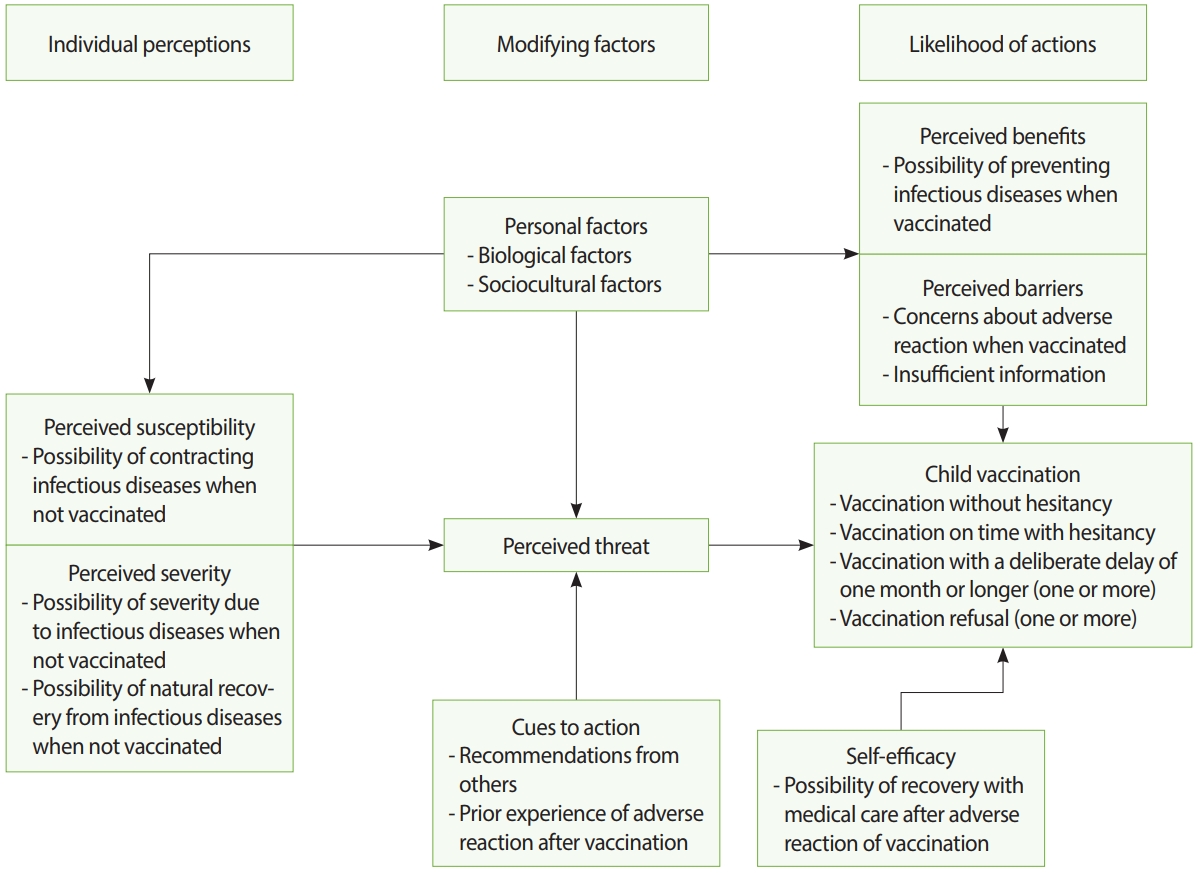
Figure 2.Levels of perception about the (A) necessity and (B) safety of child vaccinations. VH1, vaccination without hesitancy; VH2, vaccination on time with hesitancy; VH3, vaccination with a deliberate delay of one month or longer (one or more); VH4, vaccination refusal (one or more). ***p<0.001 from chi-square for trend test.

Table 1.The general characteristics of the parents by their perceptions about vaccinating children
|
Category |
Outcome |
No. of people |
VH1 |
VH2 |
VH3 |
VH4 |
p-value1
|
|
Sex |
Female |
119 |
37 (88.1) |
19 (95.0) |
32 (100) |
31 (91.2) |
0.398 |
|
Male |
9 |
5 (11.9) |
1 (5.0) |
0 (0.0) |
3 (8.8) |
|
|
No response2
|
1 |
1 |
0 |
0 |
0 |
|
|
Age (yr) |
Mean±SD |
38.1±3.7 |
37.5±3.6 |
38.9±4.0 |
38.5±4.2 |
37.8±3.2 |
0.4603
|
|
Minimum-Maximum |
28-46 |
30-46 |
29-44 |
28-46 |
32-45 |
|
|
Marital status |
Married |
125 |
41 (95.3) |
19 (95.0) |
31 (100) |
34 (100) |
0.158 |
|
Divorced or widowed |
3 |
2 (4.7) |
1 (5.0) |
0 (0.0) |
0 (0.0) |
|
|
No response2
|
1 |
0 |
0 |
1 |
0 |
|
|
Education level |
Graduated high school |
3 |
1 (2.3) |
1 (5.0) |
1 (3.1) |
0 (0.0) |
0.532 |
|
Graduated college or university |
95 |
31 (72.1) |
11 (55.0) |
26 (81.3) |
27 (79.4) |
|
|
Graduated graduate school |
31 |
11 (25.6) |
8 (40.0) |
5 (15.6) |
7 (20.6) |
|
|
Subjective income level |
Upper |
3 |
3 (7.1) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
0.006 |
|
Middle |
109 |
36 (85.7) |
19 (95.0) |
30 (93.8) |
24 (70.6) |
|
|
Lower |
14 |
3 (7.1) |
1 (5.0) |
2 (6.3) |
8 (23.5) |
|
|
No response2
|
3 |
1 |
0 |
0 |
2 |
|
|
No. of children |
1 |
47 |
17 (39.5) |
10 (50.0) |
8 (25.0) |
12 (35.3) |
0.355 |
|
2 |
69 |
22 (51.2) |
9 (45.0) |
20 (62.5) |
18 (52.9) |
|
|
3 |
13 |
4 (9.3) |
1 (5.0) |
4 (12.5) |
4 (11.8) |
|
|
Total |
|
129 (100) |
43 (33.3) |
20 (15.5) |
32 (24.8) |
34 (26.4) |
- |
Table 2.Levels of factors of the health belief model by vaccine hesitancy
|
Questions |
Agreed/respondents |
VH1 |
VH2 |
VH3 |
VH4 |
p-value1
|
|
Perceived susceptibility |
79/124 (63.7) |
39 (90.7) |
16 (80.0) |
14 (46.7) |
10 (32.3) |
<0.001 |
|
If my child does not receive the required vaccinations, she/he could be affected by infectious diseases |
|
|
|
|
|
|
|
I don’t know2
|
5 |
0 |
0 |
2 |
3 |
|
|
Perceived severity |
62/121 (51.2) |
36 (83.7) |
8 (50.0) |
11 (36.7) |
7 (21.9) |
<0.001 |
|
If my child does not receive the required vaccinations, she/he could develop a severe condition (example: inpatient treatment at a medical facility) due to infectious diseases |
|
|
|
|
|
|
|
I don’t know2
|
8 |
0 |
4 |
2 |
2 |
|
|
Even if my child does not receive the required vaccinations and is affected by infectious diseases, she/he can sufficiently recover naturally without medical treatment |
36/113 (31.9) |
6 (14.3) |
3 (20.0) |
12 (42.9) |
15 (53.6) |
<0.001 |
|
I don’t know2
|
16 |
1 |
5 |
4 |
6 |
|
|
Perceived benefits |
72/117 (61.5) |
41 (95.3) |
15 (78.9) |
12 (44.4) |
4 (14.3) |
<0.001 |
|
If my child receives the required vaccinations, infectious diseases can be effectively prevented |
|
|
|
|
|
|
|
I don’t know2
|
12 |
0 |
1 |
5 |
6 |
|
|
Perceived barriers |
104/120 (86.7) |
30 (76.9) |
16 (84.2) |
28 (93.3) |
30 (93.8) |
0.024 |
|
If my child receives the required vaccinations, adverse reactions might occur |
|
|
|
|
|
|
|
I don’t know2
|
9 |
4 |
1 |
2 |
2 |
|
|
I have not received trustable and sufficient information about the required vaccinations for my child |
88/126 (69.8) |
23 (56.1) |
12 (63.2) |
27 (84.4) |
26 (76.5) |
0.019 |
|
I don’t know2
|
3 |
2 |
1 |
0 |
0 |
|
|
Cues to action |
28/129 (21.7) |
2 (4.7) |
4 (20.0) |
11 (34.4) |
11 (32.4) |
0.001 |
|
Have your child actually had an experience of adverse reactions after receiving the required vaccination? |
|
|
|
|
|
|
|
I don’t know2
|
0 |
0 |
0 |
0 |
0 |
|
|
Have you directly or indirectly heard of cases in which the child of some- one close to you has delayed or refused the required vaccination? |
101/129 (78.3) |
25 (58.1) |
17 (85.0) |
28 (87.5) |
31 (91.2) |
<0.001 |
|
I don’t know2
|
0 |
0 |
0 |
0 |
0 |
|
|
Have you directly or indirectly heard of cases in which the child of some- one close to you has experienced adverse reactions after receiving the required vaccination? |
52/129 (40.3) |
7 (16.3) |
10 (50.0) |
18 (56.3) |
17 (50.0) |
0.001 |
|
I don’t know2
|
0 |
0 |
0 |
0 |
0 |
|
|
Self-efficacy |
54/102 (52.9) |
27 (81.8) |
10 (62.5) |
9 (34.6) |
8 (29.6) |
<0.001 |
|
Even if my child experiences adverse reactions due to required vac- cinations, she/he can recover through sufficient medical treatment |
|
|
|
|
|
|
|
I don’t know2
|
27 |
10 |
4 |
6 |
7 |
|
|
Total |
129 (100) |
43 (100) |
20 (100) |
32 (100) |
34 (100) |
|
Table 3.Results of a logistic regression analysis on the factors of vaccine hesitancy
|
Questions |
|
Unadjusted |
Adjusted1
|
|
Perceived severity |
|
|
|
|
If my child does not receive the required vaccinations, she/he could develop a severe condition (example: inpatient treatment at a medical facility) due to infectious diseases. |
Disagree |
1.0 (reference) |
1.0 (reference) |
|
Agree |
7.2 (3.2, 16.0) |
6.5 (1.1, 38.9) |
|
Even if my child does not receive the required vaccinations and is affected by infectious diseases, she/he can sufficiently recover naturally without medical treatment. |
Disagree |
1.0 (reference) |
1.0 (reference) |
|
Agree |
5.0 (2.1, 12.0) |
1.3 (0.2, 7.4) |
|
Perceived benefits |
|
|
|
|
If my child receives the required vaccinations, infectious diseases can be effectively prevented. |
Agree |
1.0 (reference) |
1.0 (reference) |
|
Disagree |
22.8 (8.2, 63.3) |
5.0 (0.9, 28.6) |
|
Perceived barriers |
|
|
|
|
If my child receives the required vaccinations, adverse reactions might occur. |
Disagree |
1.0 (reference) |
1.0 (reference) |
|
Agree |
3.8 (1.1, 12.5) |
2.7 (0.4, 18.1) |
|
I have not received trustable and sufficient information about the required vaccinations for my child. |
Disagree |
1.0 (reference) |
1.0 (reference) |
|
Agree |
2.9 (1.3, 6.4) |
1.0 (0.2, 4.8) |
|
Cue to action |
|
|
|
|
Have your child actually had an experience of adverse reactions after receiving the required vaccination? |
No |
1.0 (reference) |
1.0 (reference) |
|
Yes |
4.8 (1.8, 12.7) |
2.0 (0.2, 19.3) |
|
Have you directly or indirectly heard of cases in which the child of someone close to you has delayed or refused the required vaccination? |
No |
1.0 (reference) |
1.0 (reference) |
|
Yes |
4.2 (1.6, 10.8) |
4.1 (0.6, 28.0) |
|
Have you directly or indirectly heard of cases in which the child of someone close to you has experienced adverse reactions after receiving the required vaccination? |
No |
1.0 (reference) |
1.0 (reference) |
|
Yes |
3.1 (1.5, 6.4) |
3.4 (0.6, 20.0) |
|
Self-efficacy |
|
|
|
|
Even if my child experiences adverse reactions due to required vaccinations, she/he can recover through sufficient medical treatment. |
Agree |
1.0 (reference) |
1.0 (reference) |
|
Disagree |
6.5 (2.7, 15.6) |
1.3 (0.2, 7.4) |
Table 4.Reasons for vaccine hesitancy
|
Reasons for vaccine hesitancy |
Classification by vaccine hesitancy (responded “yes”)1
|
|
VH2 |
VH3 |
VH4 |
|
Because I do not think that vaccination meaningfully prevents infectious diseases |
4 (20.0) |
12 (38.7) |
20 (58.8) |
|
Because of concerns about the adverse reactions caused by vaccinations or because of prior experiences with small or large adverse reactions |
13 (65.0) |
22 (68.8) |
25 (75.8) |
|
Because I cannot trust the vaccination policies of the government |
5 (25.0) |
17 (53.1) |
18 (54.5) |
|
Because I cannot trust the vaccination safety management of pharmaceutical companies and medical institutions |
10 (50.0) |
15 (46.9) |
22 (68.8) |
|
Because of religious beliefs |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Because I trust Korean traditional medicine or alternative medicine more than modern medical science, or because of naturalistic beliefs |
3 (15.0) |
7 (21.9) |
7 (21.2) |
|
Total |
20 (100) |
32 (100) |
43 (100) |
Table 5.Person(s) who had an impact on vaccine hesitancy
|
Person(s) who had an impact on the vaccine hesitancy |
Classification by vaccine hesitancy (responded with “yes”)1
|
|
VH1 |
VH2 |
VH3 |
|
Family (spouse, parents, male siblings, female siblings, cousins, etc.) |
1 (5.0) |
11 (34.4) |
6 (17.6) |
|
Acquaintances (friends, colleagues, neighbors, etc.) |
8 (40.0) |
11 (34.4) |
18 (52.9) |
|
Leaders or activists of a joined organization (social groups, civil society groups, etc.) |
2 (10.0) |
6 (18.8) |
13 (39.4) |
|
Leaders or activists of a joined organization (religious group) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Anti-vaccination activists whom I found through web, blogs, social network services, and broadcasts |
11 (55.0) |
12 (37.5) |
18 (54.5) |
|
Experts of Korean traditional medicine or alternative medicine |
1 (5.0) |
8 (25.0) |
10 (30.3) |
|
Decision made by myself |
10 (50.0) |
25 (78.1) |
25 (75.8) |
|
Total |
20 (100) |
32 (100) |
43 (100) |
REFERENCES
- 1. Edwards KM, Hackell JM; Committee on Infectious Diseases, & Committee on Practice and Ambulatory Medicine. Countering vaccine hesitancy. Pediatrics 2016;138:e20162146.ArticlePubMed
- 2. Blume S. Anti-vaccination movements and their interpretations. Soc Sci Med 2006;62:628-642.ArticlePubMed
- 3. McIntosh ED, Janda J, Ehrich JH, Pettoello-Mantovani M, Somekh E. Vaccine hesitancy and refusal. J Pediatr 2016;175:248-249.ArticlePubMed
- 4. Lo NC, Hotez PJ. Public health and economic consequences of vaccine hesitancy for measles in the United States. JAMA Pediatr 2017;171:887-892.ArticlePubMedPMC
- 5. Tsuchiya Y, Shida N, Izumi S, Ogasawara M, Kakinuma W, Tsujiuchi T, et al. Factors associated with mothers not vaccinating their children against mumps in Japan. Public Health 2016;137:95-105.ArticlePubMed
- 6. Sandhofer MJ, Robak O, Frank H, Kulnig J. Vaccine hesitancy in Austria: a cross-sectional survey. Wien Klin Wochenschr 2017;129:59-64.ArticlePubMedPDF
- 7. World Health Organization. Report of the SAGE working group on vaccine hesitancy; 2014 [cited 2019 Jul 8]. Available from: https://www.who.int/immunization/sage/meetings/2014/october/SAGE_working_group_revised_report_vaccine_hesitancy.pdf.
- 8. Di Pietro ML, Poscia A, Teleman AA, Maged D, Ricciardi W. Vaccine hesitancy: parental, professional and public responsibility. Ann Ist Super Sanita 2017;53:157-162.PubMed
- 9. Clarke S, Giubilini A, Walker MJ. Conscientious objection to vaccination. Bioethics 2017;31:155-161.ArticlePubMed
- 10. Parasidis E, Opel DJ. Parental refusal of childhood vaccines and medical neglect laws. Am J Public Health 2017;107:68-71.ArticlePubMedPMC
- 11. Chung Y, Schamel J, Fisher A, Frew PM. Influences on immunization decision-making among US parents of young children. Matern Child Health J 2017;21:2178-2187.ArticlePubMedPMCPDF
- 12. McClure CC, Cataldi JR, O’Leary ST. Vaccine hesitancy: where we are and where we are going. Clin Ther 2017;39:1550-1562.ArticlePubMed
- 13. Larson HJ, de Figueiredo A, Xiahong Z, Schulz WS, Verger P, Johnston IG, et al. The state of vaccine confidence 2016: global insights through a 67-country survey. EBioMedicine 2016;12:295-301.ArticlePubMedPMC
- 14. Park B, Choi EJ, Park B, Han H, Cho SJ, Choi HJ, et al. Factors influencing vaccination in Korea: findings from focus group interviews. J Prev Med Public Health 2018;51:173-180.ArticlePubMedPMCPDF
- 15. Brennan JM, Bednarczyk RA, Richards JL, Allen KE, Warraich GJ, Omer SB. Trends in personal belief exemption rates among alternative private schools: Waldorf, Montessori, and holistic kindergartens in California, 2000–2014. Am J Public Health 2017;107:108-112.ArticlePubMedPMC
- 16. Hayden JA. Introduction to health behavior theory. 2nd ed. Sudbury: Jones & Bartlett Learning; 2013. p 63-71.
- 17. Donadiki EM, Jiménez-García R, Hernández-Barrera V, Sourtzi P, Carrasco-Garrido P, López de Andrés A, et al. Health Belief Model applied to non-compliance with HPV vaccine among female university students. Public Health 2014;128:268-273.ArticlePubMed
- 18. Smith PJ, Humiston SG, Marcuse EK, Zhao Z, Dorell CG, Howes C, et al. Parental delay or refusal of vaccine doses, childhood vaccination coverage at 24 months of age, and the Health Belief Model. Public Health Rep 2011;126 Suppl 2:135-146.ArticlePubMed
- 19. Carrion ML. An ounce of prevention: identifying cues to (in) action for maternal vaccine refusal. Qual Health Res 2018;28:2183-2194.ArticlePubMed
- 20. Smith LE, Weinman J, Amlôt R, Yiend J, Rubin GJ. Parental expectation of side effects following vaccination is self-fulfilling: a prospective cohort study. Ann Behav Med 2019;53:267-282.ArticlePubMedPDF
- 21. Bryden GM, Browne M, Rockloff M, Unsworth C. Anti-vaccination and pro-CAM attitudes both reflect magical beliefs about health. Vaccine 2018;36:1227-1234.ArticlePubMed
- 22. Jung M. Challenges of vaccinations in the era of new media communication. Health Care Manag (Frederick) 2018;37:142-146.ArticlePubMed
- 23. Carpiano RM, Fitz NS. Public attitudes toward child undervaccination: a randomized experiment on evaluations, stigmatizing orientations, and support for policies. Soc Sci Med 2017;185:127-136.ArticlePubMed
- 24. Brelsford D, Knutzen E, Neher JO, Safranek S. Clinical inquiries: which interventions are effective in managing parental vaccine refusal? J Fam Pract 2017;66:E12-E14.PubMed
- 25. Bocquier A, Fressard L, Cortaredona S, Zaytseva A, Ward J, Gautier A, et al. Social differentiation of vaccine hesitancy among French parents and the mediating role of trust and commitment to health: a nationwide cross-sectional study. Vaccine 2018;36:7666-7673.ArticlePubMed
- 26. McKee C, Bohannon K. Exploring the reasons behind parental refusal of vaccines. J Pediatr Pharmacol Ther 2016;21:104-109.ArticlePubMedPMC
- 27. Cordrey K, McLaughlin L, Das P, Milanaik R. Pediatric resident education and preparedness regarding vaccine-preventable diseases. Clin Pediatr (Phila) 2018;57:327-334.ArticlePubMed
- 28. Marshall GS, O’Leary ST. Dismissal policies for vaccine refusal. JAMA Pediatr 2018;172:1101.Article
- 29. Lee S, Riley-Behringer M, Rose JC, Meropol SB, Lazebnik R. Parental vaccine acceptance: a logistic regression model using previsit decisions. Clin Pediatr (Phila) 2017;56:716-722.ArticlePubMed
- 30. Lee C, Whetten K, Omer S, Pan W, Salmon D. Hurdles to herd immunity: distrust of government and vaccine refusal in the US, 2002-2003. Vaccine 2016;34:3972-3978.ArticlePubMed
- 31. Attwell K, Navin MC, Lopalco PL, Jestin C, Reiter S, Omer SB. Recent vaccine mandates in the United States, Europe and Australia: a comparative study. Vaccine 2018;36:7377-7384.ArticlePubMed
- 32. Rosen JB, Arciuolo RJ, Khawja AM, Fu J, Giancotti FR, Zucker JR. Public health consequences of a 2013 measles outbreak in New York City. JAMA Pediatr 2018;172:811-817.ArticlePubMedPMC
- 33. Colgrove J. Vaccine refusal revisited—the limits of public health persuasion and coercion. N Engl J Med 2016;375:1316-1317.ArticlePubMed
- 34. Rozbroj T, Lyons A, Lucke J. Psychosocial and demographic characteristics relating to vaccine attitudes in Australia. Patient Educ Couns 2019;102:172-179.ArticlePubMed
- 35. Larson HJ. Vaccine trust and the limits of information. Science 2016;353:1207-1208.ArticlePubMed
Citations
Citations to this article as recorded by

- Ideological differences in COVID-19 vaccine intention: the effects of trust in the healthcare system, in complementary and alternative medicine, and perceived threat from the disease
Monika Lamot, Katja Kerman, Andrej Kirbiš
Frontiers in Psychology.2024;[Epub] CrossRef - Evaluation of the Attitudes of Vaccination-hesitant Parents Towards Complementary and Alternative Medicine
Hilal Koyuncu, Ayşegül Bükülmez, Ayşe Oflu
Güncel Pediatri.2024; 22(1): 58. CrossRef - Çocukluk Çağı Asılarının Kabulünü Etkileyen Faktörlerin İncelenmesi: Aşı Reddi
Reyhan AYDIN DOĞAN, Yılmaz ALTUNER, Yıldız ÖĞÜTÜCÜ, Nazlıcan AYDOĞDU, Zeynep ELLİALTIOĞLU, İrem TUNÇ, Hilal ZORLU
Sağlık Akademisi Kastamonu.2023;[Epub] CrossRef - Toplumdaki Bireylerin Aşı Uygulamalarına Karşı Tutumları ile Covid-19 Salgını Sonrası Tutumlarının Belirlenmesi
Berna BAYIR, Fatma Nur YAĞIZ, Rabia ÇAT, Gülnur ÇAT
Adnan Menderes Üniversitesi Sağlık Bilimleri Fakültesi Dergisi.2023; 7(1): 38. CrossRef - Gap between cognitions and behaviors among children’s guardians of influenza vaccination: The role of social influence and vaccine-related knowledge
Jing Wu, Zheng Wei, Yingying Yang, Xiu Sun, Siyi Zhan, Qijing Jiang, Chuanxi Fu
Human Vaccines & Immunotherapeutics.2023;[Epub] CrossRef - Maternal perceptions of vaccinating boys against human papillomavirus (HPV) in Seoul, South Korea: A descriptive exploratory qualitative study
Jihye Choi, Christine Markham, Irene Tamí-Maury, Sooyoun Kim, Paula Cuccaro, Omar Enzo Santangelo
PLOS ONE.2023; 18(3): e0282811. CrossRef - VACCINE HESITANCY OF PARENTS AND FAMILY MEMBERS OF CHILDREN AND THE CONTROL OF IMMUNOPREVENTABLE DISEASES
Izabella da Silva Viana, Emília Gallindo Cursino, Priscila da Silva Miranda, Liliane Faria da Silva, Maria Estela Diniz Machado
Cogitare Enfermagem.2023;[Epub] CrossRef - HESITAÇÃO VACINAL DE PAIS E FAMILIARES DE CRIANÇAS E O CONTROLE DAS DOENÇAS IMUNOPREVENÍVEIS
Izabella da Silva Viana, Emília Gallindo Cursino, Priscila da Silva Miranda, Liliane Faria da Silva, Maria Estela Diniz Machado
Cogitare Enfermagem.2023;[Epub] CrossRef - VACILACIÓN VACUNAL ENTRE LOS PADRES Y FAMILIARES DE LOS NIÑOS Y LA LUCHA CONTRA LAS ENFERMEDADES INMUNOPREVENIBLES
Izabella da Silva Viana, Emília Gallindo Cursino, Priscila da Silva Miranda, Liliane Faria da Silva, Maria Estela Diniz Machado
Cogitare Enfermagem.2023;[Epub] CrossRef - Hesitação vacinal em crianças menores de cinco anos: revisão de escopo
Eugênio Barbosa de Melo Júnior, Priscilla Dantas Almeida, Beatriz Mourão Pereira, Paulo de Tarso Moura Borges, Elucir Gir, Telma Maria Evangelista de Araújo
Revista Brasileira de Enfermagem.2023;[Epub] CrossRef - Vaccination hesitation in children under five years of age: a scoping review
Eugênio Barbosa de Melo Júnior, Priscilla Dantas Almeida, Beatriz Mourão Pereira, Paulo de Tarso Moura Borges, Elucir Gir, Telma Maria Evangelista de Araújo
Revista Brasileira de Enfermagem.2023;[Epub] CrossRef - An Integrative Review of the Influence on Human Papillomavirus Vaccination Adherence among Adolescents
Hyewon Shin, Sunyeob Choi, Ju-Young Lee
Healthcare.2023; 11(18): 2534. CrossRef - Vaccine hesitancy and emerging parental norms: A qualitative study in Taiwan
Chen‐I Kuan
Sociology of Health & Illness.2022; 44(3): 692. CrossRef - A systematic literature review to clarify the concept of vaccine hesitancy
Daphne Bussink-Voorend, Jeannine L. A. Hautvast, Lisa Vandeberg, Olga Visser, Marlies E. J. L. Hulscher
Nature Human Behaviour.2022; 6(12): 1634. CrossRef - Models of determinants of COVID-19 vaccine hesitancy in non-pregnant and pregnant population: Review of current literature”
Lauren Tostrud, Julia Thelen, Anna Palatnik
Human Vaccines & Immunotherapeutics.2022;[Epub] CrossRef - Addressing COVID-19 vaccine hesitancy: A content analysis of government social media platforms in England and Italy during 2020–2021
Giulia Sesa, Katarzyna Czabanowska, Antonio Giangreco, John Middleton
Public Health in Practice.2022; 4: 100345. CrossRef - Çocukluk Çağı Aşı Tereddüdü ile Karşılaşma Sıklığı, Nedenleri ve Çözüm Önerileri: Samsun İli Aile Sağlığı Merkezlerindeki Sağlık Çalışanlarıyla Kesitsel Bir Çalışma
Mehtap ALTUNTAŞ, Mustafa Kürşat ŞAHİN
Turkish Journal of Family Medicine and Primary Care.2022; 16(4): 761. CrossRef - Physical and mental health characteristics related to trust in and intention to receive COVID-19 vaccination: results from a Korean community-based longitudinal study
Ye Jin Jeon, Youngrong Lee, Ji Su Yang, Young Su Park, Sun Jae Jung
Epidemiology and Health.2022; 44: e2022064. CrossRef - Paradoxical health care utilization patterns among children in Korea who did not receive mandatory pneumococcal vaccination
Sangho Sohn, Kwan Hong, Hari Hwang, Byung Chul Chun
Vaccine.2021; 39(7): 1096. CrossRef - Differential Demographic and Clinical Characteristics between MMR Vaccinated and Unvaccinated Children in South Korea: A Nationwide Study
Dongwon Yoon, Juhwan Kim, Juyoung Shin
Vaccines.2021; 9(6): 653. CrossRef - Determinants of parental hesitancy to vaccinate their children against COVID-19 in China
Mei-Xian Zhang, Xiao-Qing Lin, Yan Chen, Tao-Hsin Tung, Jian-Sheng Zhu
Expert Review of Vaccines.2021; 20(10): 1339. CrossRef - Aşı Karşıtı Tutumların Sosyokültürel ve Dinî Boyutları
Talip DEMİR
Tevilat.2021; 2(2): 271. CrossRef - Examination of parents refusing administration of childhood vaccinations: Turkey example
Caner Baysan, Seher Palanbek Yavaş, Mehmet Uğur Karabat
CHILD`S HEALTH.2021; 16(3): 218. CrossRef - Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: a large-scale retrospective temporal modelling study
Alexandre de Figueiredo, Clarissa Simas, Emilie Karafillakis, Pauline Paterson, Heidi J Larson
The Lancet.2020; 396(10255): 898. CrossRef - World Outbreak Trend of Infectious Diseases with Surveillance
Soo-Yeon Choi, Jung Heon Kim, Jiyeon Kim, Eung-Soo Hwang
Journal of Bacteriology and Virology.2019; 49(3): 141. CrossRef

 , Soon Young Lee
, Soon Young Lee
 PubReader
PubReader ePub Link
ePub Link Cite
Cite