
Articles
- Page Path
- HOME > Epidemiol Health > Volume 45; 2023 > Article
-
Original Article
Association between PM2.5 exposure and risk of Parkinson’s disease in individuals with chronic obstructive pulmonary disease in Taiwan: a nested case-control study -
Ci-Wen Luo1,2*
 , Yu-Hsiang Kuan2,3*, Wen-Ying Chen4, Chun-Jung Chen5, Frank Cheau-Feng Lin6,7, Stella Chin-Shaw Tsai8,9
, Yu-Hsiang Kuan2,3*, Wen-Ying Chen4, Chun-Jung Chen5, Frank Cheau-Feng Lin6,7, Stella Chin-Shaw Tsai8,9 -
Epidemiol Health 2023;45:e2023094.
DOI: https://doi.org/10.4178/epih.e2023094
Published online: October 17, 2023
1Department of Medical Research, Tungs’ Taichung MetroHarbor Hospital, Taichung, Taiwan
2Department of Pharmacology, Chung Shan Medical University School of Medicine, Taichung, Taiwan
3Department of Pharmacy, Chung Shan Medical University Hospital, Taichung, Taiwan
4Department of Veterinary Medicine, National Chung Hsing University, Taichung, Taiwan
5Department of Education and Research, Taichung Veterans General Hospital, Taichung, Taiwan
6Department of Thoracic Surgery, Chung Shan Medical University Hospital, Taichung, Taiwan
7School of Medicine, Chung Shan Medical University, Taichung, Taiwan
8Superintendent Office, Tungs’ Taichung MetroHarbor Hospital, Taichung, Taiwan
9Department of Post-Baccalaureate Medicine, National Chung Hsing University College of Medicine, Taichung, Taiwan
- Correspondence: Stella Chin-Shaw Tsai Superintendent Office, Tungs’ Taichung MetroHarbor Hospital, 699 Section 8, Taiwan Boulevard, Taichung 43503, Taiwan E-mail: t5722@ms3.sltung.com.tw
- Co-correspondence: Frank Cheau-Feng Lin Department of Thoracic Surgery, Chung Shan Medical University Hospital, 110 Section 1, Jianguo North Road, Taichung 40201, Taiwan E-mail: frnklin@gmail.com
- *Luo & Kuan contributed equally to this work as joint first authors.
© 2023, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,122 Views
- 113 Download
Abstract
-
OBJECTIVES
- This cohort study investigated the correlation between Parkinson’s disease (PD) risk and chronic obstructive pulmonary disease (COPD) risk under particulate matter with an aerodynamic diameter ≤2.5 μm (PM2.5) exposure.
-
METHODS
- Data from the National Health Research Institutes of Taiwan were used in this study. The Environmental Protection Administration of Taiwan established an air quality monitoring network for monitoring Taiwan’s general air quality. COPD was indicated by at least 3 outpatient records and 1 hospitalization for COPD. After the implementation of age, sex, and endpoint matching at a 1:4 ratio, 137 patients and 548 patients were included in the case group and control group, respectively. Based on the 2005 World Health Organization (WHO) standards, monthly air particle concentration data were classified into the following 4 groups in analyses of exposure–response relationships: normal level, and 1.0, 1.5, and 2.0 times the WHO level ([concentration ≥2]×25 μg/m3×number of exposure months).
-
RESULTS
- A multivariate logistic regression revealed that the 1.0 and 1.5 WHO level groups did not significantly differ from the normal level group, but the 2.0 WHO level did (odds ratio, 4.091; 95% confidence interval, 1.180 to 14.188; p=0.038).
-
CONCLUSIONS
- Elevated PM2.5 concentrations were significantly correlated with an increased risk of PD among patients with COPD. Furthermore, exposure to high PM2.5 levels can further increase the risk of PD.
- Parkinson’s disease (PD) is a progressive neurodegenerative disorder with a typical presentation of slow progression and accumulating disability [1]. PD-related motor impairments, such as tremor, rigidity, slowed movement, and postural instability, can increase the likelihood of falls [2]. Cognitive impairments that affect executive functions, attention, and eventual memory involvement are predictors of poor clinical outcomes and an increased risk of developing dementia [3,4]. The incidence and prevalence of PD have been increasing rapidly worldwide. The global number of individuals with PD exceeded 6 million in 2015, and this number is projected to exceed 12 million by 2040 because of aging populations worldwide [5]. To date, PD has no disease-modifying treatment. Patients with PD not only require more physician consultations and emergency department visits, but also tend to have longer hospital stays relative to their same-age peers [6].
- Chronic obstructive pulmonary disease (COPD) is a respiratory disease caused by exposure to inhaled particulate matter and a combination of multiple genetic, developmental, and social factors [7,8]. COPD is a key contributor to morbidity and mortality rates worldwide; in Taiwan, the mortality rate associated with COPD was 26.1 in every 100,000 people in 2014 [8]. For male aged > 55 years without COPD, the estimated risk of developing COPD within the next 40 years is 24% [9]. COPD is associated with numerous comorbidities, including coronary artery disease, heart failure, lung cancer, pulmonary artery disease, and malnutrition [10]. Other COPD-related comorbidities included systemic inflammatory metabolic diseases such as diabetes and hypertension and mental illnesses such as anxiety and depression [11]. A Taiwanese study also highlighted that compared with the general population, the risk of PD in patients with COPD was significantly higher [12].
- Air pollution, particularly that caused by particulate matter with an aerodynamic diameter ≤ 2.5 μm (PM2.5), is a risk factor associated with COPD. Short-term exposure to air pollution exacerbates COPD [11], and older adults are more sensitive to adverse reactions, with the estimated risk being higher in European countries than in Asian countries. Various other confounding factors also contribute to the inconsistent results [13,14]. Exposure to annual average PM2.5 in the United States is significantly associated with an increased risk of first hospitalization for PD, Alzheimer’s disease, and related dementia [15]. C57BL/6J mice have been used as an in vivo model to show that PM2.5 exposure exacerbates behavioral abnormalities in individuals with PD by increasing oxidative stress, reducing autophagy and mitophagy, and inducing mitochondrial-mediated neuronal apoptosis [16].
- Studies have suggested a relationship between greater PM2.5 exposure and higher COPD and PD risk and confirmed the higher risk of PD development in individuals with COPD. Our study aimed to investigate whether PD risk was correlated with exposure to PM2.5 in COPD patients.
INTRODUCTION
- Data sources
- This cohort study analyzed data obtained from the National Health Research Institutes of Taiwan, specifically the National Health Insurance Research Database (NHIRD). Since 1995, Taiwan’s National Health Insurance program has provided universal and publicly funded health coverage to the country’s population, which is currently approximately 23 million. This program is mandatory and covers more than 98% of Taiwan’s population [17]. The NHIRD includes records of both hospital admissions and outpatient visits, and clinicians apply the International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM), to assign codes to the data. The database has been validated by numerous studies. Because of the encryption and de-identification processes implemented by the NHIRD, patient privacy is protected.
- Collection of particulate matter with an aerodynamic diameter ≤2.5 μm concentration data
- The Environmental Protection Administration of Taiwan established an air quality monitoring network (AMQN) to monitor the general air quality in Taiwan. In this monitoring network, the PM2.5 concentration in the atmosphere is measured using a tapered element oscillating microbalance (R&P 1400; Rupprecht & Patashnick Co., New York, NY, USA) and measurements are recorded once per hour. The time interval for follow-up was measured in months, and the present study used monthly average cumulative exposure to compare the PM2.5 exposure levels of the studied patients. A patient’s exposure was determined using the exposure measurement taken at the monitoring station where the patient was located. If a patient’s location did not have a monitoring station, the patient’s exposure was determined using the measurement taken at the nearest monitoring station or the average of the 2 nearest monitoring stations. The observed air particle exposure levels that the studied patients were exposed to were determined on the basis of the monthly average cumulative exposure levels from the year 2008 to the endpoint. The hourly cumulative exposure level multiplied by 24 was used as the basis for daily exposure. If more than 8 hours of data were missing, the patient was excluded. The monthly average exposure level for a given month was calculated by multiplying the average daily exposure by the number of days in that month. If more than 10 days of data were missing, the patient was excluded. The monthly average air particle concentration at a given city was estimated and regarded as the population exposure of the city. We referenced studies that used quartiles to establish a basis for grouping exposure concentrations [18]. To analyze the exposure–response relationship, the monthly concentration of air particles was classified into the following 4 categories by applying the 2005 World Health Organization (WHO) standards: normal level (≤25 μg/m3 ×number of exposure months), 1.0 times the WHO level ([1≤ concentration< 1.5]× [25 μg/m3 × number of exposure months]), 1.5 times the WHO level (1.5≤ concentration< 2]× [25 μg/m3 × number of exposure months]), and 2.0 times the WHO level ([concentration≥ 2]× 25 μg/m3 × number of exposure months).
- Study population
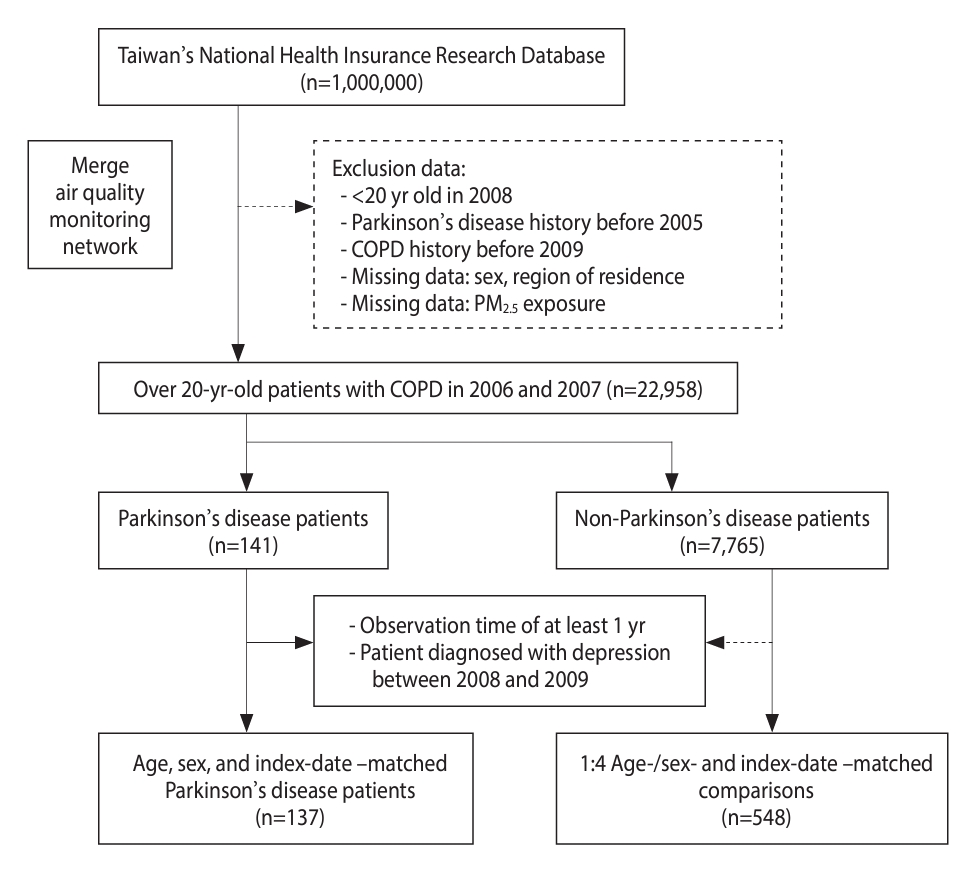
- From the NHIRD and the AQMN database, the present study obtained data on the PM2.5 exposure and population characteristics of patients with COPD for the period from 2006 to 2013. Individuals aged ≥ 20 years with no history of COPD (ICD-9 codes: 491.x, 492.x, and 496.x) prior to 2005 were enrolled between 2006 and 2007 [19]. COPD was indicated by at least 3 outpatient records and 1 hospitalization record for COPD. In total, 8,160 patients were diagnosed with COPD, and those with missing values were excluded (Figure 1). Among these patients, 141 were diagnosed with PD (ICD-9 code: 332.0), and 7,765 were undiagnosed with PD [20]. In the present nested case-control study, patients who were diagnosed with PD within 365 days between 2008 and 2009 were excluded from the case group, and their counterparts were excluded from the control group. Patients with missing PM2.5 data were also excluded from both groups. We matched the case group with a control group that was 4 times larger. After the implementation of 1:4 matching for age, sex, and index date, 137 patients and 548 patients were included in the case group and control group, respectively.
- The basic participant characteristics examined in the present study were sex, age, low income, and urbanization level. In Taiwan, households with a monthly income of < 20,000 New Taiwan dollars [21] are exempt from paying income tax. The 359 registered communities in Taiwan are divided into 7 urbanization levels based on their composite scores for population density, education level ratio, proportion of older adults aged ≥ 65 years, proportion of the community engaged in agricultural activities, and the number of individuals with COPD per 100,000 people [22]. The 7 urbanization levels are highly urbanized, moderate urbanization, emerging town, general town, aging towns, agrarian towns, and remote township. The comorbidities associated with COPD include diabetes, hypertension, ischemic stroke, fracture, depression, cancer, and Alzheimer’s disease [23].
- Statistical analysis
- We performed various statistical tests to analyze the data. The Shapiro–Wilk test was applied to identify whether the data distribution was non-normal (p< 0.05), and the Wilcoxon rank-sum test was conducted to assess differences in continuous variables between the case and control groups. The chi-square test was performed to analyze differences in categorical variables between the case and control groups. To calculate the odds ratios (ORs) and 95% confidence intervals (CIs), we used multivariate logistic regression models. These models were adjusted for potential risk factors such as PD-related comorbidities, age, sex, low income, and urbanization level. Specifically, we employed multivariate logistic regression to estimate the OR and 95% CI for PD risk in patients with COPD who were exposed to PM2.5. We performed all statistical analyses using the SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and p< 0.05 indicated statistical significance.
- Ethics statement
- The present study was approved by the Institutional Review Board of Tungs’ Taichung MetroHarbor Hospital (IRB No. 111,070).
MATERIALS AND METHODS
- Patient characteristics
- Table 1 presents the basic characteristics of PM2.5 exposure among patients in the case group (PD) and comparison group (non-PD). The patients with PD who were diagnosed with COPD between 2006 and 2007 in the NHIRD were followed up from 2008 to 2013 after matching was performed for age (±5 years), sex, and index date (±180 days). No significant difference between the case and control groups was detected for sex, age, and low income. The 2 groups also did not differ significantly with respect to urbanization level; however, a high proportion of both groups lived in highly urbanized cities, with 28.5% of the patients with PD and 26.6% of those without PD living in those areas. For comorbidities, significant between-group differences were detected for diabetes and anemia, with a significantly higher proportion of the patients with PD (diabetes, 28.4%; anemia, 16.7%) experiencing these conditions relative to the patients; thus, these were identified as risk factors for PD (diabetes, 21.6%; anemia, 11.5%).
- Particulate matter with an aerodynamic diameter ≤2.5 μm exposure as risk factor for Parkinson’s disease
- Table 2 shows the distribution of WHO PM2.5 levels among the case and control groups. The mean follow-up period was 42.42±16.79 months for the patients with PD and 42.50±16.60 months for the patients without PD. At normal levels, the median PM2.5 exposure was 1,023.57 μg/m³ (mean±standard deviation [SD], 940.96±321.74) for 13 patients with PD and 834.12 μg/m³ (mean±SD, 778.54±289.57) for 54 patients without PD. At the WHO 1.0 level, the median PM2.5 exposure was 1,354.78 μg/m³ (mean±SD, 1,315.02 ±590.59) for 80 patients with PD and 1,279.43 μg/m³ (mean±SD, 1,310.19±586.53) for 356 patients without PD. At the WHO 1.5 level, the median PM2.5 exposure was 1,426.56 μg/m³ (mean ±SD, 1,582.35 ±702.32) for 37 patients with PD and 1,746.72 μg/m³ (mean±SD, 1,723.57±683.53) for 130 patients without PD. At the WHO 2.0 level, the median PM2.5 exposure was 2,276.40 μg/m³ (mean±SD, 2,197.08±179.38) for 7 patients with PD and 2,226.65 μg/m³ (mean±SD, 2,220.99±129.18) for 8 patients without PD. The chi-square test revealed a significant difference in PM2.5 exposure levels between the PD and control groups.
- Determination of the odds ratio of particulate matter with an aerodynamic diameter ≤2.5 μm exposure level as risk factor for chronic obstructive pulmonary disease through logistic regression
- Table 3 presents the confounding variables for the risk of developing PD in patients with COPD who were exposed to PM2.5. The multivariate logistic regression revealed that the WHO 1.0 and 1.5 level groups did not significantly differ from the normal level group, but the WHO 2.0 level group did (OR, 4.091; 95% CI, 1.180 to 14.188; p= 0.026). No significant difference was observed for sex, age, and low income. PD risk did not significantly differ between areas with and without high urbanization; however, a higher trend was observed for aging towns (OR, 2.333; 95% CI, 0.868 to 6.268). Only the comorbidities of anemia (OR, 1.606; 95% CI, 0.998 to 2.584) and diabetes (OR, 1.458; 95% CI, 0.966 to 2.201) were significantly associated with PD risk.
RESULTS
- The body of evidence on the link between air pollution and neurological disorders is growing, particularly with respect to the link between ozone and particulate matter exposure and brain diseases [24]. This includes the activation of microglial cells and other inflammatory markers, elevated levels of midbrain α-synuclein protein, and the loss of dopamine neurons in the substantia nigra [25-27]. Progressive damage occurs in various regions of the brain, and such damage is accompanied by behavioral changes and small glial cell activation, changes in the morphology of the substantia nigra and striatum cells, and the loss of neurons [28,29]; these changes are similar to those observed in the brains of patients with PD [30].
- PM2.5 is a crucial contributor to the risk of not only PD, but also cardiovascular disease and other related chronic diseases such as COPD [16]. Studies have reported that exposure to PM2.5 induces lung inflammation in mice and exacerbates cigarette-smoke-induced inflammation [31]. The levels of interleukin 6 and 8 were reported to be upregulated in PM2.5-exposed cells in a dose-dependent manner, impairing the transition of AT2 cells to AT1 cells in a mouse model [31]. Various epidemiological studies have demonstrated that exposure to particulate matter pollution, including PM2.5, is associated with numerous chronic diseases in both developed and developing countries [18]. In particular, PM2.5 can pass through the blood–lung barrier and blood–brain barrier, thereby increasing the incidence of respiratory, cardiovascular, and neurodegenerative diseases [19]. The neuroinflammatory process can be attributed to the ability of PM2.5 particles to reach the nasal epithelium through respiration and to transfer to the brain through the olfactory bulb [20]. Our research findings indicated a correlation between an elevated PM2.5 concentration and an increased risk of PD among patients with COPD. Furthermore, exposure to high levels of PM2.5 can further elevate the risk of PD.
- PD is the second most common age-related neurodegenerative disorder, affecting approximately 3% and 5% of the populations aged > 65 years and > 85 years, respectively [21]. Males have a 2-fold greater risk of developing PD relative to females, but female exhibit a higher mortality rate; furthermore, COPD is more hazardous for male than for female [23,32]. In a recent meta-analysis, age-related increases in PD incidence were observed in both sexes, but males in the 60-year-old to 70-year-old age group exhibited a faster increase relative to individuals in the other age groups [24]. Our results indicated that relative to females, males constituted a larger proportion of the study population, tended to be older, and exhibited greater PD risk if they were living in an aged township, even though this trend was non-significant. However, because of the limitations related to our research methodology, we could not clarify the correlation between PD and COPD risk factors. Compared with winter births, spring births were reported to have a 30% higher risk of PD [25]. The amount of early-life sunlight exposure and subsequent vitamin D3 levels of individuals may influence their risk of developing PD [26]. In a United Kingdom study, non-motor symptoms in patients with PD exhibited seasonal fluctuations, particularly symptoms related to cardiovascular, sensory, hallucinatory, and olfactory functions, and such symptoms worsened considerably in the winter [27]. Based on the possible seasonal and sunlight-related PD trends reported by one study, we treated birth season and diagnosis season as confounding factors and made the necessary adjustments. Although differences in the number of PD cases were observed across birth and diagnosis seasons, they were non-significant.
- Numerous studies have reported that diabetes mellitus increases the risk of PD. Insulin plays a crucial role in protecting neurons during neuron development by binding to its receptors [28]. In PD cell models, insulin reduces the BAX/BAL2 ratio by activating the phosphatidylinositol-3-kinase/protein kinase B/glycogen synthase kinase 3 pathway [29]. These pathophysiological links include neuroinflammation, mitochondrial dysfunction, oxidative stress, and protein misfolding processes [30]. Insulin resistance and hyperglycemia are the underlying causes of most comorbidities related to diabetes mellitus, and they also have negative effects on PD. Oxidative stress can lead to anemia because it affects lipid peroxidation and DNA damage [33], contributing to the development of anemia under these pathological conditions [34]. The disruption of iron homeostasis can lead to various neurodegenerative diseases, including PD. A preclinical study reported that mice with gene knockout of iron-regulating proteins that regulate cell iron homeostasis developed progressive neurodegeneration [35]. Males with anemia were reported to have a higher incidence of PD; however, this trend was not observed in females, which may be related to gynecological diseases. Our results indicated that after adjustments were made, no significant relationship was detected between diabetes and anemia, which may reflect the effects of hormones [36]; however, the patients with diabetes and anemia had a higher risk for PD than their counterparts.
- The present study has several limitations. First, no laboratory data were collected. Data pertaining to biochemical markers such as eosinophil count and glycosylated hemoglobin levels could not be collected from the patients. However, adjustments were made for comorbidity-related confounding factors to minimize the influence of this limitation on our results. Second, the patients’ PM2.5 exposure data could be inaccurate to some extent. PM2.5 exposure was determined on the basis of the patients’ residential areas; however, some patients spent time in other areas during the study period, which would have affected their exposure to PM2.5. However, for long-term exposure, the patients’ main activity areas were likely to be close to their place of residence; thus, this limitation did not have a substantial effect on our results. Third, the details of the patients’ lifestyle habits (such as smoking and drinking) are not recorded in the NHIRD, and lifestyle-related factors could have influenced the results. However, we adjusted for socioeconomic status, comorbidities, and urbanization level, and these factors did not lead to significant deviations from our results.
- The present study identified a concentration-dependent relationship between PM2.5 exposure and the risk of PD in patients with COPD, with a higher concentration of PM2.5 leading to a greater risk of PD. These results highlight the necessity of considering neurodegenerative diseases in the context of environmental pollution and respiratory symptoms.
DISCUSSION
-
DATA AVAILABILITY
All data generated or examined during this research are incorporated within this article.
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This study was supported by research grants from National Science and Technology Council of Taiwan (NSTC 111-2,314-B-040 -008; 109-2,320-B-040-MY3). Tungs’ Taichung MetroHarbor Hospital (grant No. TTMHH-R1120,009), the National Chung Hsing University and Chung Shan Medical University (NCHUCSMU-11,110), and the Chung Shan Medical University Hospital (CSH-2,022-C-028).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Luo CW, Kuan YH, Lin FCF, Tsai SCS. Data curation: Kuan YH, Chen WY, Chen CJ. Formal analysis: Luo CW, Lin FCF, Tsai SCS. Funding acquisition: Chen WY, Kuan YH, Lin FCF, Tsai SCS. Methodology: Luo CW, Kuan YH. Project administration: Kuan YH, Lin FCF, Tsai SCS. Visualization: Luo CW, Chen WY, Chen CJ. Writing – original draft: Luo CW, Chen WY, Chen CJ. Writing – review & editing: Kuan YH, Lin FCF, Tsai SCS.
NOTES
ACKNOWLEDGEMENTS
| PM2.5 exposure level | n (%) |
Distribution of PM2.5 (μg/m3) |
p-value1 | ||||
|---|---|---|---|---|---|---|---|
| Mean±SD | Q1 | Median | Q3 | ||||
| Parkinson’s disease (follow-up: 42.42±16.79 mo) | 0.048 | ||||||
| Normal level | 13 (9.5) | 940.96±321.74 | 663.57 | 1,023.57 | 1,138.76 | ||
| 1.0 WHO level | 80 (58.4) | 1,315.02±590.59 | 807.72 | 1,354.78 | 1,735.38 | ||
| 1.5 WHO level | 37 (27.0) | 1,582.35±702.32 | 1,073.75 | 1,426.56 | 2,066.99 | ||
| 2.0 WHO level | 7 (5.1) | 2,197.08±179.38 | 2,007.95 | 2,276.40 | 2,375.88 | ||
| Non-Parkinson’s disease (follow-up: 42.50±16.60 mo) | |||||||
| Normal level | 54 (9.8) | 778.54± 289.57 | 578.25 | 834.12 | 967.49 | ||
| 1.0 WHO level | 356 (65.0) | 1,310.19±586.53 | 815.17 | 1,279.43 | 1,736.23 | ||
| 1.5 WHO level | 130 (23.7) | 1,723.57±683.53 | 1,147.51 | 1,746.72 | 2,291.85 | ||
| 2.0 WHO level | 8 (1.5) | 2,220.99±129.18 | 2,148.92 | 2,226.65 | 2,326.14 | ||
- 1. Bloem BR, Okun MS, Klein C. Parkinson’s disease. Lancet 2021;397:2284-2303.ArticlePubMed
- 2. Opara J, Małecki A, Małecka E, Socha T. Motor assessment in Parkinson`s disease. Ann Agric Environ Med 2017;24:411-415.ArticlePubMed
- 3. Zhang Q, Aldridge GM, Narayanan NS, Anderson SW, Uc EY. Approach to cognitive impairment in Parkinson’s disease. Neurotherapeutics 2020;17:1495-1510.ArticlePubMedPMCPDF
- 4. Aarsland D, Batzu L, Halliday GM, Geurtsen GJ, Ballard C, Ray Chaudhuri K, et al. Parkinson disease-associated cognitive impairment. Nat Rev Dis Primers 2021;7:47.ArticlePubMedPDF
- 5. Dorsey ER, Bloem BR. The Parkinson pandemic-a call to action. JAMA Neurol 2018;75:9-10.ArticlePubMed
- 6. Ng JS. Palliative care for Parkinson’s disease. Ann Palliat Med 2018;7:296-303.ArticlePubMed
- 7. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet 2022;399:2227-2242.ArticlePubMed
- 8. Cheng SL, Lin CH, Chu KA, Chiu KL, Lin SH, Lin HC, et al. Update on guidelines for the treatment of COPD in Taiwan using evidence and GRADE system-based recommendations. J Formos Med Assoc 2021;120:1821-1844.ArticlePubMed
- 9. Crisafulli E, Costi S, Luppi F, Cirelli G, Cilione C, Coletti O, et al. Role of comorbidities in a cohort of patients with COPD undergoing pulmonary rehabilitation. Thorax 2008;63:487-492.ArticlePubMed
- 10. Cavaillès A, Brinchault-Rabin G, Dixmier A, Goupil F, Gut-Gobert C, Marchand-Adam S, et al. Comorbidities of COPD. Eur Respir Rev 2013;22:454-475.ArticlePubMedPMC
- 11. Putcha N, Drummond MB, Wise RA, Hansel NN. Comorbidities and chronic obstructive pulmonary disease: prevalence, influence on outcomes, and management. Semin Respir Crit Care Med 2015;36:575-591.ArticlePubMedPMC
- 12. Li CH, Chen WC, Liao WC, Tu CY, Lin CL, Sung FC, et al. The association between chronic obstructive pulmonary disease and Parkinson’s disease: a nationwide population-based retrospective cohort study. QJM 2015;108:39-45.ArticlePubMed
- 13. Arbex MA, de Souza Conceição GM, Cendon SP, Arbex FF, Lopes AC, Moysés EP, et al. Urban air pollution and chronic obstructive pulmonary disease-related emergency department visits. J Epidemiol Community Health 2009;63:777-783.ArticlePubMed
- 14. Zhu RX, Nie XH, Chen YH, Chen J, Wu SW, Zhao LH. Relationship between particulate matter (PM2.5) and hospitalizations and mortality of chronic obstructive pulmonary disease patients: a meta-analysis. Am J Med Sci 2020;359:354-364.ArticlePubMed
- 15. Shi L, Wu X, Danesh Yazdi M, Braun D, Abu Awad Y, Wei Y, et al. Long-term effects of PM2· 5 on neurological disorders in the American Medicare population: a longitudinal cohort study. Lancet Planet Health 2020;4:e557-e565.ArticlePubMedPMC
- 16. Wang Y, Li C, Zhang X, Kang X, Li Y, Zhang W, et al. Exposure to PM2.5 aggravates Parkinson’s disease via inhibition of autophagy and mitophagy pathway. Toxicology 2021;456:152770.ArticlePubMed
- 17. Wu TY, Majeed A, Kuo KN. An overview of the healthcare system in Taiwan. London J Prim Care (Abingdon) 2010;3:115-119.ArticlePubMedPMC
- 18. Sun HY, Luo CW, Chiang YW, Yeh KL, Li YC, Ho YC, et al. Association between PM2.5 exposure level and primary open-angle glaucoma in Taiwanese adults: a nested case-control study. Int J Environ Res Public Health 2021;18:1714.ArticlePubMedPMC
- 19. Gothe H, Rajsic S, Vukicevic D, Schoenfelder T, Jahn B, GeigerGritsch S, et al. Algorithms to identify COPD in health systems with and without access to ICD coding: a systematic review. BMC Health Serv Res 2019;19:737.ArticlePubMedPMCPDF
- 20. Swarztrauber K, Anau J, Peters D. Identifying and distinguishing cases of parkinsonism and Parkinson’s disease using ICD-9 CM codes and pharmacy data. Mov Disord 2005;20:964-970.ArticlePubMed
- 21. Lee YF. Economic growth and income inequality: the modern Taiwan experience. J Contemp China 2008;17:361-374.Article
- 22. Lin YJ, Tian WH, Chen CC. Urbanization and the utilization of outpatient services under National Health Insurance in Taiwan. Health Policy 2011;103:236-243.ArticlePubMed
- 23. Santiago JA, Bottero V, Potashkin JA. Biological and clinical implications of comorbidities in Parkinson’s disease. Front Aging Neurosci 2017;9:394.ArticlePubMedPMC
- 24. Block ML, Elder A, Auten RL, Bilbo SD, Chen H, Chen JC, et al. The outdoor air pollution and brain health workshop. Neurotoxicology 2012;33:972-984.ArticlePubMedPMC
- 25. Campbell A, Oldham M, Becaria A, Bondy SC, Meacher D, Sioutas C, et al. Particulate matter in polluted air may increase biomarkers of inflammation in mouse brain. Neurotoxicology 2005;26:133-140.ArticlePubMed
- 26. Levesque S, Surace MJ, McDonald J, Block ML. Air pollution & the brain: subchronic diesel exhaust exposure causes neuroinflammation and elevates early markers of neurodegenerative disease. J Neuroinflammation 2011;8:105.ArticlePubMedPMCPDF
- 27. Levesque S, Taetzsch T, Lull ME, Kodavanti U, Stadler K, Wagner A, et al. Diesel exhaust activates and primes microglia: air pollution, neuroinflammation, and regulation of dopaminergic neurotoxicity. Environ Health Perspect 2011;119:1149-1155.ArticlePubMedPMC
- 28. Angoa-Pérez M, Jiang H, Rodríguez AI, Lemini C, Levine RA, Rivas-Arancibia S. Estrogen counteracts ozone-induced oxidative stress and nigral neuronal death. Neuroreport 2006;17:629-633.ArticlePubMed
- 29. Santiago-López D, Bautista-Martínez JA, Reyes-Hernandez CI, Aguilar-Martínez M, Rivas-Arancibia S. Oxidative stress, progressive damage in the substantia nigra and plasma dopamine oxidation, in rats chronically exposed to ozone. Toxicol Lett 2010;197:193-200.ArticlePubMed
- 30. Kirrane EF, Bowman C, Davis JA, Hoppin JA, Blair A, Chen H, et al. Associations of ozone and PM2.5 concentrations with Parkinson’s disease among participants in the agricultural health study. J Occup Environ Med 2015;57:509-517.ArticlePubMedPMC
- 31. Wu TY, Majeed A, Kuo KN. An overview of the healthcare system in Taiwan. London J Prim Care (Abingdon) 2010;3:115-119.ArticlePubMedPMC
- 32. Lin YJ, Tian WH, Chen CC. Urbanization and the utilization of outpatient services under National Health Insurance in Taiwan. Health Policy 2011;103(2-3):236-243.ArticlePubMed
- 33. Madhikarmi NL, Murthy KR. Antioxidant enzymes and oxidative stress in the erythrocytes of iron deficiency anemic patients supplemented with vitamins. Iran Biomed J 2014;18:82-87.PubMedPMC
- 34. Bissinger R, Bhuyan AA, Qadri SM, Lang F. Oxidative stress, eryptosis and anemia: a pivotal mechanistic nexus in systemic diseases. FEBS J 2019;286:826-854.ArticlePubMedPDF
- 35. Ghosh MC, Zhang DL, Rouault TA. Iron misregulation and neurodegenerative disease in mouse models that lack iron regulatory proteins. Neurobiol Dis 2015;81:66-75.ArticlePubMedPMC
- 36. Marras C, Saunders-Pullman R. The complexities of hormonal influences and risk of Parkinson’s disease. Mov Disord 2014;29:845-848.ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

