Articles
- Page Path
- HOME > Epidemiol Health > Volume 45; 2023 > Article
-
Original Article
Exploring cognitive trajectories and their association with physical performance: evidence from the China Health and Retirement Longitudinal Study -
Jingdong Suo1,2
 , Xianlei Shen1,2, Jinyu He1,2, Haoran Sun1,2, Yu Shi1,2, Rongxin He1,2, Xiao Zhang1,2, Xijie Wang1,2, Yuandi Xi1,2,3, Wannian Liang1,2
, Xianlei Shen1,2, Jinyu He1,2, Haoran Sun1,2, Yu Shi1,2, Rongxin He1,2, Xiao Zhang1,2, Xijie Wang1,2, Yuandi Xi1,2,3, Wannian Liang1,2 -
Epidemiol Health 2023;45:e2023064.
DOI: https://doi.org/10.4178/epih.e2023064
Published online: July 9, 2023
1Vanke School of Public Health, Tsinghua University, Beijing, China
2Institute for Healthy China, Tsinghua University, Beijing, China
3Beijing Key Laboratory of Environmental Toxicology, School of Public Health, Capital Medical University, Beijing, China
- Correspondence: Wannian Liang Vanke School of Public Health Tsinghua University, 30 Shuangqing Road, Beijing 100084, China E-mail: liangwn@tsinghua.edu.cn
- Co-correspondence: Xijie Wang Vanke School of Public Health Tsinghua University, 30 Shuangqing Road, Beijing 100084, China E-mail: xijie_wang@126.com
© 2023, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
OBJECTIVES
- The long-term trends of cognitive function and its associations with physical performance remain unclear, particularly in Asian populations. The study objectives were to determine cognitive trajectories in middle-aged and elderly Chinese individuals, as well as to examine differences in physical performance across cognitive trajectory groups.
-
METHODS
- Data were extracted from the China Health and Retirement Longitudinal Study. A total of 5,701 participants (47.7% male) with a mean age of 57.8 (standard deviation, 8.4) years at enrollment were included. A group-based trajectory model was used to identify cognitive trajectory groups for each sex. Grip strength, repeated chair stand, and standing balance tests were used to evaluate physical performance. An ordered logistic regression model was employed to analyze differences in physical performance across cognitive trajectory groups.
-
RESULTS
- Three cognitive trajectory groups were identified for each sex: low, middle, and high. For both sexes, higher cognitive trajectory groups exhibited smaller declines with age. In the fully adjusted model, relative to the low trajectory group, the odds ratios (ORs) of better physical performance in the middle cognitive group were 1.37 (95% confidence interval [CI], 1.17 to 1.59; p<0.001) during follow-up and 1.40 (95% CI, 1.20 to 1.64; p<0.001) at the endpoint. The ORs in the high trajectory group were 1.94 (95% CI, 1.61 to 2.32; p<0.001) during follow-up and 2.04 (95% CI, 1.69 to 2.45; p<0.001) at the endpoint.
-
CONCLUSIONS
- Cognitive function was better preserved in male participants and individuals with higher baseline cognitive function. A higher cognitive trajectory was associated with better physical performance over time.
- The global population and life expectancy are growing, leading to an escalating aging problem. In 2018, 249 million individuals in China were aged 60 and older, accounting for 17.9% of the total population [1]. By 2050, this population is projected to exceed 450 million, representing a share of over 30% [2]. However, the increase in healthy life expectancy has been much slower than that of overall life expectancy [3], resulting in a rapid rise in age-related diseases.
- A growing public health concern, aging is associated with declines in bodily functions and physical performance [4]. Previous studies have demonstrated that a decrease in physical performance often marks the early stages of disability in older individuals [5]. Poor physical performance has been consistently linked to adverse health risks, including total and cause-specific mortality [6], depression [7], falls [8], frailty [9], and hospitalization [10]. However, the indicators of physical performance vary across studies and can include grip strength, standing balance, gait speed, functional reach tests, and chair stands. Although it is widely accepted that maintaining good physical performance in old age is important, further research is required to better understand its longitudinal and overall development.
- Cognitive impairment is an early stage of dementia, determined by a wide variety of neurological, psychological, and emotional factors [11,12]. The rapid aging process increases the burden of age-related cognitive decline, which occurs in many areas, including memory storage, emotional control, processing speed, and decision-making [12]. Currently, 50 million people worldwide are estimated to have dementia, and this number is expected to reach 81.1 million by 2040 [13]. Rather than relying on single observations, long-term follow-up and identification of cognitive trajectory constitute approaches for investigating cognitive changes over time, along with the determinants of such changes [14]. However, since relatively few studies have examined the cognitive trajectories of middle-aged and elderly people, the population-based phenotypes of cognitive change remain unclear.
- Recently, studies have demonstrated that changes in cognitive function are associated with physical performance in the areas of mobility [15], balance [16], and muscle strength [17]. However, these findings primarily stem from single-center, cross-sectional studies with relatively small sample sizes, and they vary depending on the study design [15,18]. Consequently, we sought to investigate the progression of cognitive function over time and its association with physical performance using a multicenter, nationally representative cohort in China.
- Utilizing data from the 2011, 2013, and 2015 waves of the China Health and Retirement Longitudinal Study (CHARLS), this study was conducted with the goal of identifying diverse patterns of cognitive trajectories and examining their associations with physical performance outcomes in middle-aged and elderly populations.
INTRODUCTION
- Study participants
- The data for this study was obtained from the CHARLS, a nationally representative prospective cohort survey conducted by the National School of Development at Peking University. The baseline survey took place in 2011 and was followed by 2 additional surveys in 2013 and 2015, utilizing a multistage probability sampling design and a probability-proportional-to-size sampling technique [19]. The CHARLS included thousands of participants aged 45 years and older from 150 counties/districts and 450 villages/resident committees across 28 provinces in China, with a large sample size, strong representation, and high data quality. Personal information, mental and physical health data, and basic family information were collected during each wave of the survey.
- In the present study, participants who completed all 3 waves of surveying were included (7,697 of 16,381; 47.0%). Among these individuals, those with incomplete demographic information (n=36), missing physical performance indicators (no responses for all 4 measurements, n=891), and incomplete cognitive function measurements (missing more than 6 items, n=1,069) were excluded. Consequently, 5,701 participants were included in the data analysis.
- Physical performance measurement
- Physical performance was considered to be indicated by grip strength, repeated chair stands, and 2 standing balance tests. Each of these indicators was assigned a score of either 0 or 1, depending on whether they were completed successfully. The total physical performance score was calculated by summing the scores of the 3 indicators, and this was done at baseline, during follow-up, and at the endpoint. The physical performance score ranged from 0 to 3.
- Grip strength, an indicator of upper limb muscle strength, was measured using a dynamometer (Yuejian WL-1000; Nantong Yuejian Physical Measurement Instrument Co., Ltd., Nantong, China) and recorded in kilograms [6,19]. During testing, participants were asked to stand (unless physically precluded from doing so), hold the dynamometer at a right angle, squeeze the handle as hard as possible for a few seconds, and then release. Grip strength for each hand was tested twice in an alternating manner, and the average of the 4 tests was recorded [20]. For 556 participants with 1 missing test, the average of the other completed tests was used for the analysis. Participants were assigned 1 point if the score was above the median and 0 points if it was not.
- Repeated chair stands, an indicator of lower limb muscle strength, were assessed using a standard chair with a height of 47 centimeters from the floor [21]. Participants were instructed to sit in the chair with their arms folded across their chest, then to stand up straight and sit back down as quickly as possible 5 times without stopping or using their arms for assistance. A score of 1 point was given if the participant successfully completed the test, and a score of 0 points was given otherwise.
- The standing balance test, which evaluates static balance, endurance, and postural control ability, was assessed using semitandem stands and full-tandem stands [22]. In the semi-tandem stand test, participants were required to stand with the side of the heel of one foot touching the big toe of the other foot for 10 seconds without losing balance, moving the feet, or touching anything. For the full-tandem stand test, participants were instructed to stand with the heel of one foot in front of and touching the toes of the other foot. A 30-second full-tandem stand test was used for participants aged 70 years or older, while a 60-second full-tandem stand test was used for those under 70 years old. Participants were awarded 1 point if they successfully completed both tests and 0 points if they did not.
- Cognitive assessment
- Cognitive function in the CHARLS was assessed across 2 dimensions, evaluating orientation, attention, visuospatial abilities, and word recall [23,24]. The mental status dimension incorporated information from the Telephone Interview of Cognitive Status, which included orientation, numeric ability, and visuospatial abilities. Orientation was assessed by asking respondents to provide the date, season, and day of the week (5 points). Numeric ability was measured by having respondents subtract 7 from 100 five consecutive times (5 points). Visuospatial abilities were evaluated by presenting respondents with a picture and asking them to redraw the image just shown (1 point). The episodic memory dimension involved collecting data on immediate word recall (10 points) and delayed word recall (10 points). The total cognitive function score was calculated by summing the scores from each dimension, with a possible range of 0 points (worst) to 31 points (best).
- Covariates
- Baseline socio-demographic characteristics and health-related factors were considered for the adjusted analysis. Socio-demographic characteristics included age, sex (male or female), residence (urban or rural), province (of 28 provinces), marital status (married or not), and education level (illiterate, elementary school, or middle school and above). Residence was defined based on China’s National Bureau of Statistics, with urban areas including cities, city suburbs, towns, town suburbs, and other special zones, while all other areas were considered rural [19,25]. For marital status, individuals were considered married if they were either living with their spouse or temporarily separated due to reasons such as work. Regarding education level, respondents were classified as illiterate if they had no formal education or did not complete primary school, while all others were categorized as having completed elementary school or higher. Health-related factors included body mass index (BMI), smoking status (yes/no), drinking status (yes/no), and diagnosis of chronic non-communicable diseases (yes/no).
- Statistical analysis
- We utilized group-based trajectory modeling to identify distinct trajectory groups of cognitive function as they relate to age [27]. Trajectories were modeled using a censored normal distribution by sex, with age in years serving as the measure of time. The bestfit model was determined based on the following 4 criteria: (1) the Bayesian information criterion of the alternative model decreased by at least 20 relative to the previous model; (2) the odds of correct classification, a measure of assignment accuracy, exceeded 5; (3) the average posterior probability for each group was greater than 0.7; and (4) the sample size of each group constituted at least 5% of the total. Given that cognitive trajectories may differ by sex, we conducted sex-specific modeling. Initially, we modeled adherence using 2 groups to 5 groups with all cubic models to determine the most appropriate number of groups with adequate sample sizes. Subsequently, we tested the best-fit shape of cognitive trajectories. The final models consisted of 3 trajectory groups for each sex, labeled as low, middle, and high based on the value and change in cognitive function scores.
- To assess whether the socio-demographic characteristics and health influence factors differed among the 3 cognitive trajectory groups, the chi-square test was employed for categorical variables, while the independent-samples t-test was utilized for continuous variables. Physical performance was an ordinal categorical variable with a score range of 0 to 3, determined by 3 independent measures of 0 or 1 on grip strength, repeated chair stands, and standing balance tests. An ordered logistic regression model was used to analyze the differences in physical performance of participants from the 3 cognitive trajectory groups at baseline, during follow-up, and at the endpoint, using the low trajectory group as the reference. Odds ratios (ORs) and 95% confidence intervals (CIs) of physical performance for each cognitive trajectory group were calculated. Age, marital status, education level, BMI, smoking status, and drinking status were included in adjusted model 1. The presence of chronic diseases, categorized as cardiovascular and cerebrovascular metabolic diseases, psychiatric and neurological diseases, and other diseases, was incorporated into adjusted model 2. Considering that 556 (9.7%) respondents had missing grip strength data due to 1-handed disability or inconvenience, sensitivity analyses were conducted on respondents with complete grip strength data in adjusted model 3 to avoid the manifestation of poor physical performance. All analytical procedures were stratified by sex and residential status. Additionally, we analyzed the relationship between the cognitive trajectory group and each original variable of physical performance to avoid ceiling effects.
- All statistical analyses were conducted using Stata version 14.0 (StataCorp., College Station, TX, USA). An association was deemed significant if the associated 2-sided p-value was less than 0.05.
- Ethics statement
- The study was approved by the Ethical Review Committee of Peking University (No. IRB00001052-11014), and all participants provided written informed consent.
MATERIALS AND METHODS
Grip strength
Repeated chair stands
Standing balance test
- Baseline characteristics of respondents
- A total of 5,701 middle-aged and elderly Chinese individuals participated in this study (47.7% male; 21.0% from urban areas), with an average baseline age of 57.8 years (standard deviation, 8.4). Male participants demonstrated higher grip strength than female participants (36.9±8.5 vs. 25.3±6.7 kg, p<0.001) and performed more successful repeated chair stands (86.0 vs. 75.9%, p<0.001). The baseline cognitive function scores were 16.1±4.6 for male participants and 14.3±5.4 for female participants. Demographic characteristics and lifestyle information of the participants at baseline, by sex, are presented in Table 1.
- Characteristics of follow-up assessments by cognitive trajectory group
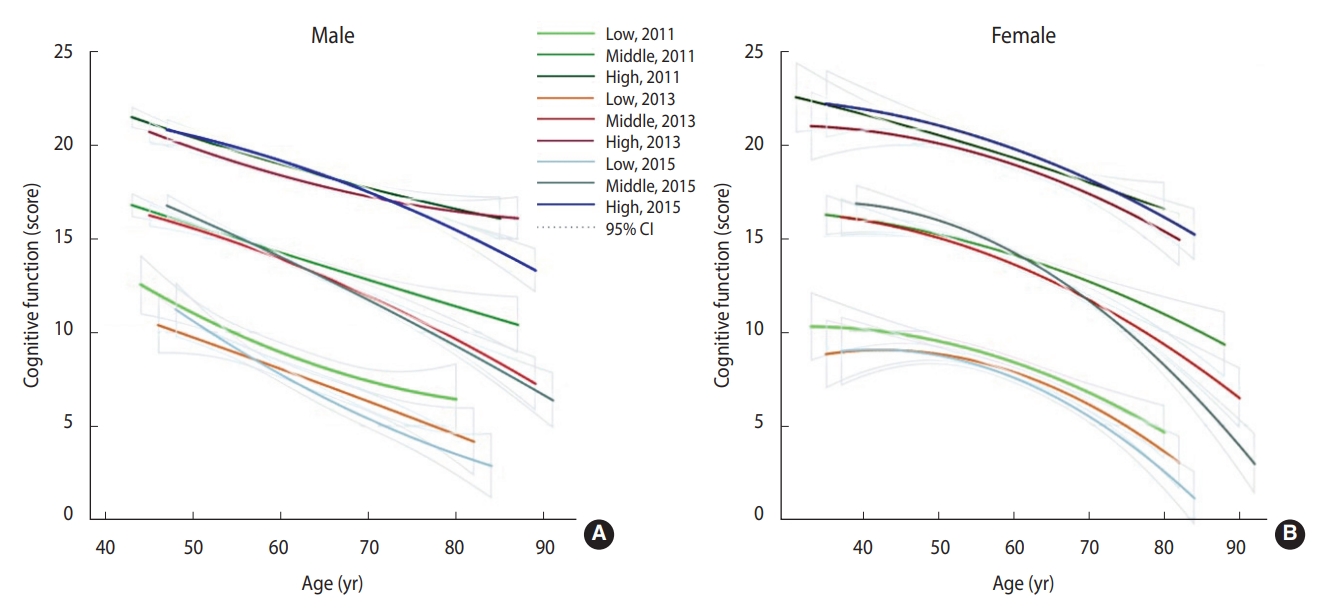
- The distribution of cognitive function scores for each cognitive trajectory group during the follow-up period is displayed in Figure 1 by sex. According to the best-fit model of group-based trajectory modeling, respondents were divided into 3 groups: 1,104 (19.4%) were in the low group (10.4% male vs. 26.9% female), 2,478 (43.5%) were in the middle group (42.4% male vs. 44.8% female), and 2,119 (37.2%) were in the high group (47.3% male vs. 28.3% female). Overall, the high group performed best in maintaining cognitive function, while the middle group exhibited the greatest cognitive change with age. Female individuals had better cognitive function than male participants at baseline, but they experienced a steeper decline with age.
- Table 2 presents the characteristics of the respondents by cognitive trajectory group. Significant differences were observed among the 3 cognitive trajectory groups in terms of sex, residence, marital status, education level, smoking status, alcohol consumption, and BMI. However, no statistical difference in age was observed among the 3 groups. Physical performance at each follow-up differed significantly among the 3 groups (p<0.001), with the group exhibiting higher cognitive function demonstrating better physical performance.
- Differences in physical performance among cognitive trajectory groups
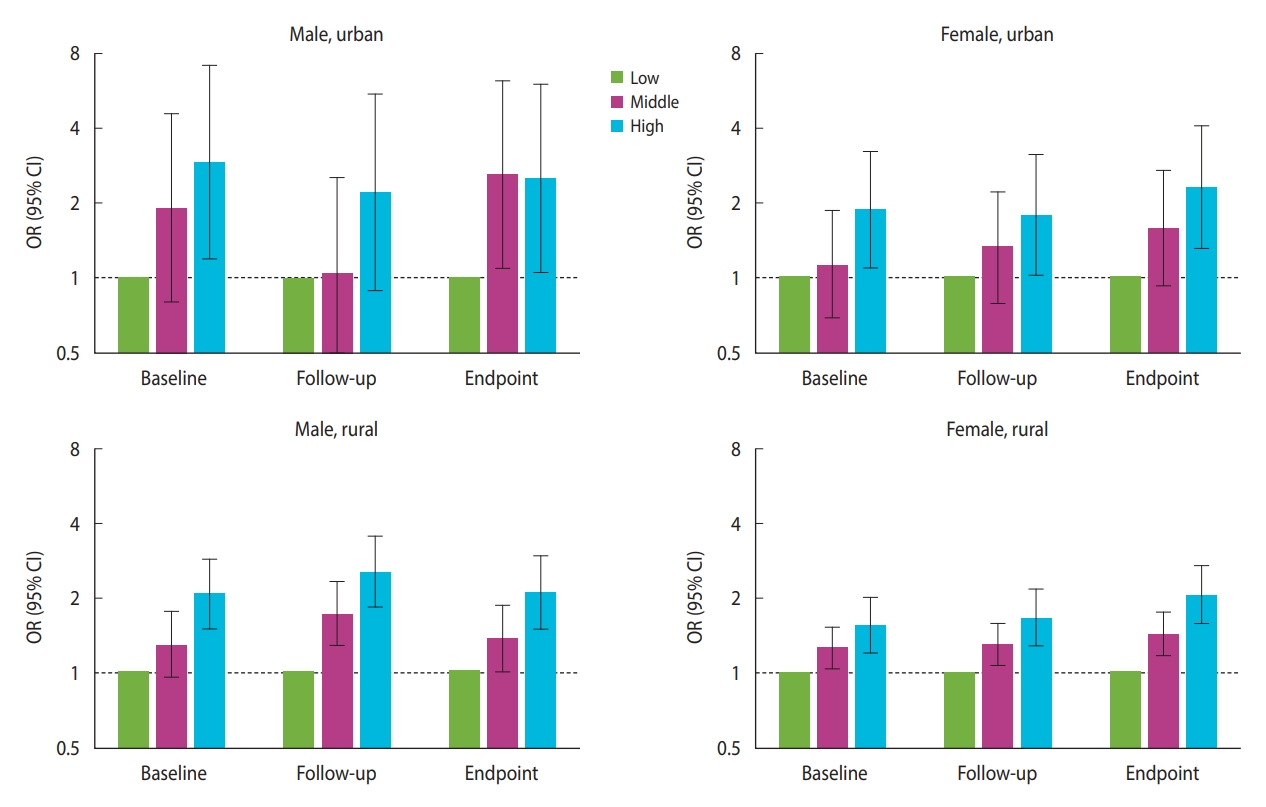
- In the fully adjusted model, compared to the low group, the ORs of better physical performance in the middle and high groups at baseline were as follows: 1.92 (95% CI, 0.80 to 4.57; p=0.142) and 2.92 (95% CI, 1.19 to 7.15; p=0.019) for urban male, 1.12 (95% CI, 0.68 to 1.86; p=0.648) and 1.86 (95% CI, 1.08 to 3.23; p=0.026) for urban female, 1.28 (95% CI, 0.95 to 1.73; p=0.108) and 2.07 (95% CI, 1.48 to 2.88; p<0.001) for rural male, and 1.25 (95% CI, 1.02 to 1.53; p=0.030) and 1.55 (95% CI, 1.18 to 2.02; p<0.001) for rural female. During follow-up, the ORs of better physical performance in the middle and high groups were 1.04 (95% CI, 0.43 to 2.53; p=0.923) and 2.21 (95% CI, 0.89 to 5.50; p=0.089) for urban male, 1.32 (95% CI, 0.78 to 2.21; p=0.297) and 1.77 (95% CI, 1.01 to 3.12; p=0.047) for urban female, 1.71 (95% CI, 1.27 to 2.31; p<0.001) and 2.53 (95% CI, 1.82 to 3.52; p<0.001) for rural male, and 1.30 (95% CI, 1.06 to 1.58; p=0.010) and 1.67 (95% CI, 1.28 to 2.18; p<0.001) for rural female. At the endpoint, the ORs of better physical performance in the middle and high groups were 2.60 (95% CI, 1.09 to 6.22; p=0.032) and 2.53 (95% CI, 1.05 to 6.10; p=0.038) for urban male, 1.57 (95% CI, 0.92 to 2.69; p=0.097) and 2.31 (95% CI, 1.30 to 4.11; p=0.004) for urban female, 1.36 (95% CI, 1.00 to 1.86; p=0.054) and 2.09 (95% CI, 1.48 to 2.95; p<0.001) for rural male, and 1.42 (95% CI, 1.16 to 1.74; p<0.001) and 2.06 (95% CI, 1.57 to 2.71; p<0.001) for rural female (Figure 2, Supplementary Material 1). All trends between the 3 cognitive trajectory groups were statistically significant (p<0.05), except for the urban male group at the endpoint. The crude model and adjusted model 1 are displayed in Supplementary Materials 2 and 3. Upon analyzing each original indicator of physical performance, the trends of grip strength and repeated chair stands between the 3 cognitive trajectory groups were all statistically significant (p<0.05). However, the results of the standing balance test showed no statistical significance (Supplementary Material 4).
- Sensitivity analyses
- Sensitivity analyses were performed for respondents with complete grip strength data, separated by sex and residential status (Supplementary Material 5). The results remained consistent with the analysis of all participants.
RESULTS
- In this study, we conducted a 4-year follow-up with 5,701 middle-aged and elderly individuals and observed a significant overall decline in cognitive function as they aged. We identified 3 distinct cognitive trajectories, which we labeled as low (19.4%), middle (43.5%), and high (37.2%). All 3 cognitive trajectories displayed parallel downward trends with age, suggesting that cognitive impairment is a chronic and irreversible degenerative pathological process [27]. We discovered that participants with higher cognitive trajectories exhibited better physical performance, and this difference became more pronounced over time. This supports previous research findings that better cognitive function is associated with better physical performance [28,29]. These associations remained significant after adjusting for covariates and in sensitivity analyses.
- Our findings demonstrated that participants with better cognitive function at baseline tended to maintain a more stable level of cognitive function as they aged. This trend was consistent with the results of previous regional studies conducted among American and Mexican populations [30,31]. Additionally, higher BMI may be a protective factor against cognitive impairment [32]. Using a nationally representative cohort survey in China, we were the first to report sex differences in cognitive trajectories among an Asian population. We also discovered that while females generally had higher cognitive levels than males, their cognitive function fluctuated and decreased more significantly with age. The results of previous studies are controversial regarding sex differences in cognitive function with age. Although research in American and European populations has indicated that female have higher initial scores on most types of cognitive tests [33,34], no definite result exists regarding whether the rate of decline differs between males and females [33,35,36]. Additional longitudinal studies focusing on Asian populations would help to clarify this pattern [32].
- The finding that a decline in overall cognitive function is associated with a decline in physical performance aligns with previous studies [28,29,37]. Prior research has shown that physical performance can predict declines in cognitive function or the risk of mild cognitive impairment and dementia later in life [38,39]. One potential mechanism is that vascular or degenerative damage to the brain, such as that caused by smoking or low hemoglobin level [40,41], may impact both cognitive and motor areas, thus explaining the link between cognitive function and physical performance. Even after adjusting for potential confounding factors, such as smoking status, drinking status, and the presence of multiple chronic diseases, we observed significant correlations between cognitive function and physical performance, particularly in grip strength and repeated stand-up tests.
- The differences in physical performance between cognitive trajectory groups also widened among female participants over time, while those in male participants remained stable. However, the underlying mechanism requires further exploration. After stratifying by urban-rural residence, we found that urban participants were more likely to be categorized into the high cognitive trajectory group, while rural participants were more likely to be assigned to the middle-low cognitive groups. This, coupled with the facts that cognitive function declined more rapidly in the lower trajectory groups to which rural participants were more likely to be assigned [42] and that rural participants were more vulnerable due to a lack of education, household wealth, and health insurance [43,44], suggests that greater attention should be paid to slowing down cognitive decline in rural areas.
- The present study had several potential limitations. First, although we found that the group with a higher cognitive trajectory exhibited better physical performance, the causal relationship and mechanism underlying this transition remain unknown and warrant further research. Second, while factors such as residence, sex, age, marital status, BMI, smoking, drinking, and chronic diseases were included in our analysis to control for confounding effects, other influential factors such as socioeconomic status and sleep duration could not be incorporated due to the design of the original CHARLS study. Third, approximately 60% of respondents from the original CHARLS dataset had missing values for key information such as cognitive function and grip strength and were therefore excluded from the present analysis. This exclusion may also impact the effect size and generalizability of our findings. Nonetheless, the CHARLS is a database that covers 150 counties/districts and 450 villages/residential committees in 28 provinces of China and possesses strong national representativeness. The relationship between physical performance and cognitive trajectory groups identified in the present study still provides a reliable basis for further research.
- Using CHARLS data, we discovered that improved cognitive function was associated with male sex, urban residency, high BMI, and high cognitive trajectory. Participants from the high cognitive trajectory group demonstrated better physical performance, suggesting that early interventions to maintain stable cognitive function may be crucial for preserving optimal physical performance in middle-aged and elderly individuals.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplement Material 1.
Supplement Material 2.
Supplement Material 3.
Supplement Material 4.
Supplement Material 5.
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This study was funded by the Sanming Project of Medicine in Shenzhen (No. SZSM202111001) and the National Natural Science Foundation of China (grant No. 82204067).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Suo J, Zhang X. Data curation: Suo J, He J. Formal analysis: Suo J, He R, Sun H. Funding acquisition: Liang W. Methodology: Shen X, Xi Y. Project administration: Wang X, Liang W. Visualization: Wang X, Shi Y. Writing - original draft: Suo J, Shen X, He J, Sun H, Shi Y. Writing - review & editing: Suo J, He R, Zhang X, Wang X, Xi Y, Liang W.
NOTES
ACKNOWLEDGEMENTS


| Characteristics | Overall | Male | Female | p for difference1 | |
|---|---|---|---|---|---|
| No. of participants | 5,701 (100) | 2,718 (47.7) | 2,983 (52.3) | - | |
| Area of residence, urban | 1,195 (21.0) | 543 (20.0) | 652 (21.9) | 0.082 | |
| Age (yr) | 57.8±8.4 | 59.3±8.3 | 56.5±8.2 | <0.001 | |
| Marital status, married | 5,156 (90.4) | 2,496 (91.8) | 2,660 (89.2) | <0.001 | |
| Education level | <0.001 | ||||
| Illiterate | 1,358 (23.8) | 294 (10.8) | 1,064 (35.7) | - | |
| Elementary school | 2,514 (44.1) | 1,289 (47.4) | 1,225 (41.1) | - | |
| ≥Middle school | 1,829 (32.1) | 1,135 (41.8) | 694 (23.3) | - | |
| Smoking, yes | 2,235 (39.2) | 2,039 (75.0) | 196 (6.6) | <0.001 | |
| Drinking, yes | 1,909 (33.5) | 1,550 (57.0) | 359 (12.0) | <0.001 | |
| Body mass index (kg/m2) | 23.6±3.9 | 23.1±3.6 | 24.2±4.0 | <0.001 | |
| Cardiovascular and cerebrovascular metabolic diseases | 2,067 (36.3) | 1,021 (37.6) | 1,046 (35.1) | 0.050 | |
| Neurological and psychiatric disorders | 149 (2.6) | 65 (2.4) | 84 (2.8) | 0.310 | |
| Other diseases | 2,825 (49.6) | 1,366 (50.3) | 1,459 (48.9) | 0.310 | |
| Physical performance | |||||
| Grip strength (kg) | 30.8±9.6 | 36.9±8.5 | 25.3±6.7 | <0.001 | |
| Repeated chair stands | 4,599 (80.7) | 2,336 (86.0) | 2,263 (75.9) | <0.001 | |
| Standing balance test | 5,681 (99.7) | 2,708 (99.6) | 2,973 (99.7) | 0.835 | |
| Cognitive function | 15.1±5.1 | 16.1±4.6 | 14.3±5.4 | <0.001 | |
| Variables | Overall |
Cognitive trajectory |
p for difference1 | ||||
|---|---|---|---|---|---|---|---|
| Low | Middle | High | |||||
| No. of participants | 5,701 (100) | 1,104 (19.4) | 2,478 (43.5) | 2,119 (37.2) | - | ||
| Sex, male | 2,718 (47.7) | 287 (26.0) | 1,150 (46.4) | 1,281 (60.5) | <0.001 | ||
| Resident, urban | 1,195 (30.0) | 115 (10.4) | 401 (16.2) | 679 (32.0) | <0.001 | ||
| Baseline | |||||||
| Age (yr) | 57.8±8.4 | 57.9±7.9 | 57.6±8.6 | 58.0±8.4 | 0.276 | ||
| Marital status, married | 5,156 (90.4) | 954 (86.4) | 2,236 (90.2) | 1,966 (92.8) | <0.001 | ||
| Education level | <0.001 | ||||||
| Illiterate | 1,358 (23.8) | 689 (62.4) | 587 (23.7) | 82 (3.9) | - | ||
| Elementary school | 2,514 (44.1) | 365 (33.1) | 1,276 (51.5) | 873 (41.2) | - | ||
| ≥Middle school | 1,829 (32.1) | 50 (4.5) | 615 (24.8) | 1,164 (54.9) | - | ||
| Smoking, yes | 2,235 (39.2) | 294 (26.6) | 961 (38.8) | 980 (46.3) | <0.001 | ||
| Drinking, yes | 1,909 (33.5) | 251 (22.7) | 786 (31.7) | 872 (41.2) | <0.001 | ||
| Body mass index (kg/m2) | 23.63±3.85 | 23.16±3.77 | 23.56±3.90 | 23.96±3.81 | <0.001 | ||
| Physical performance | 2.30±0.69 | 2.03±0.68 | 2.26±0.69 | 2.47±0.64 | <0.001 | ||
| Cognitive function | 15.13±5.15 | 8.71±3.60 | 14.39±3.53 | 19.35±3.19 | <0.001 | ||
| Follow-up | |||||||
| Physical performance | 2.30±0.69 | 2.02±0.69 | 2.28±0.69 | 2.48±0.64 | <0.001 | ||
| Cognitive function | 14.32±5.18 | 7.70±3.56 | 13.63±3.46 | 18.59±3.16 | <0.001 | ||
| Endpoint | |||||||
| Physical performance | 2.31±0.68 | 2.03±0.70 | 2.29±0.67 | 2.49±0.62 | <0.001 | ||
| Cognitive function | 14.32±5.58 | 7.02±3.66 | 13.56±3.74 | 18.95±3.28 | <0.001 | ||
- 1. National Bureau of Statistics of China. Statistical Communiqué of the People’s Republic of China on the 2018 national economic and social development; 2019 [cited 2019 May 5]. Available from: http://www.stats.gov.cn/english/PressRelease/201902/t20190228_1651335.html.
- 2. United Nations. World population prospects: the 2012 revision. [cited 2019 Jan 17]. Available from: http://esa.un.org/unpd/wpp/Excel-Data/population.htm.
- 3. Fouweather T, Gillies C, Wohland P, Van Oyen H, Nusselder W, Robine JM, et al. Comparison of socio-economic indicators explaining inequalities in Healthy Life Years at age 50 in Europe: 2005 and 2010. Eur J Public Health 2015;25:978-983.ArticlePubMed
- 4. Calder PC, Carding SR, Christopher G, Kuh D, Langley-Evans SC, McNulty H. A holistic approach to healthy ageing: how can people live longer, healthier lives? J Hum Nutr Diet 2018;31:439-450.ArticlePubMedPDF
- 5. Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med 1995;332:556-561.ArticlePubMedPMC
- 6. Nofuji Y, Shinkai S, Taniguchi Y, Amano H, Nishi M, Murayama H, et al. Associations of walking speed, grip strength, and standing balance with total and cause-specific mortality in a general population of Japanese elders. J Am Med Dir Assoc 2016;17:184.e1-184.e7.ArticlePubMed
- 7. Ganasarajah S, Sundström Poromaa I, Thu WP, Kramer MS, Logan S, Cauley JA, et al. Objective measures of physical performance associated with depression and/or anxiety in midlife Singaporean women. Menopause 2019;26:1045-1051.ArticlePubMed
- 8. Lauretani F, Ticinesi A, Gionti L, Prati B, Nouvenne A, Tana C, et al. Short-Physical Performance Battery (SPPB) score is associated with falls in older outpatients. Aging Clin Exp Res 2019;31:1435-1442.ArticlePubMedPDF
- 9. Smith G, Avenell A, Band MM, Hampson G, Lamb EJ, Littleford RC, et al. Associations between frailty, physical performance, and renal biomarkers in older people with advanced chronic kidney disease. Eur Geriatr Med 2021;12:943-952.ArticlePubMedPMCPDF
- 10. Negm AM, Kennedy CC, Pritchard JM, Ioannidis G, Vastis V, Marr S, et al. The short performance physical battery is associated with one-year emergency department visits and hospitalization. Can J Aging 2019;38:507-511.ArticlePubMed
- 11. Sanford AM. Mild cognitive impairment. Clin Geriatr Med 2017;33:325-337.ArticlePubMed
- 12. Wu MS, Lan TH, Chen CM, Chiu HC, Lan TY. Socio-demographic and health-related factors associated with cognitive impairment in the elderly in Taiwan. BMC Public Health 2011;11:22.ArticlePubMedPMCPDF
- 13. Ferri CP, Prince M, Brayne C, Brodaty H, Fratiglioni L, Ganguli M, et al. Global prevalence of dementia: a Delphi consensus study. Lancet 2005;366:2112-2117.ArticlePubMedPMC
- 14. Small BJ, Bäckman L. Longitudinal trajectories of cognitive change in preclinical Alzheimer’s disease: a growth mixture modeling analysis. Cortex 2007;43:826-834.ArticlePubMed
- 15. O’Keefe JA, Robertson EE, Ouyang B, Carns D, McAsey A, Liu Y, et al. Cognitive function impacts gait, functional mobility and falls in fragile X-associated tremor/ataxia syndrome. Gait Posture 2018;66:288-293.ArticlePubMedPMC
- 16. Meunier CC, Smit E, Fitzpatrick AL, Odden MC. Balance and cognitive decline in older adults in the cardiovascular health study. Age Ageing 2021;50:1342-1348.ArticlePubMedPMCPDF
- 17. Sui SX, Williams LJ, Holloway-Kew KL, Hyde NK, Pasco JA. Skeletal muscle health and cognitive function: a narrative review. Int J Mol Sci 2020;22:255.ArticlePubMedPMC
- 18. Donoghue O, Feeney J, O’Leary N, Kenny RA. Baseline mobility is not associated with decline in cognitive function in healthy community-dwelling older adults: findings from the Irish Longitudinal Study on Ageing (TILDA). Am J Geriatr Psychiatry 2018;26:438-448.ArticlePubMed
- 19. Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol 2014;43:61-68.ArticlePubMedPMC
- 20. Zuo M, Gan C, Liu T, Tang J, Dai J, Hu X. Physical predictors of cognitive function in individuals with hypertension: evidence from the CHARLS basline survey. West J Nurs Res 2019;41:592-614.ArticlePubMedPDF
- 21. Millor N, Lecumberri P, Gómez M, Martínez-Ramírez A, Izquierdo M. An evaluation of the 30-s chair stand test in older adults: frailty detection based on kinematic parameters from a single inertial unit. J Neuroeng Rehabil 2013;10:86.ArticlePubMedPMCPDF
- 22. Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol 1994;49:M85-M94.ArticlePubMed
- 23. Lei X, Smith JP, Sun X, Zhao Y. Gender differences in cognition in China and reasons for change over time: evidence from CHARLS. J Econ Ageing 2014;4:46-55.ArticlePubMedPMC
- 24. Luo Y, Pan X, Zhang Z. Productive activities and cognitive decline among older adults in China: evidence from the China Health and Retirement Longitudinal Study. Soc Sci Med 2019;229:96-105.ArticlePubMed
- 25. National Bureau of Statistics. China statistical yearbook 2021. Beijing: China Statistics Press; 2021.
- 26. Jones BL, Nagin DS. A note on a Stata plugin for estimating groupbased trajectory models. Sociol Methods Res 2013;42:608-613.ArticlePDF
- 27. Zhang T, Han Y, Wang J, Hou D, Deng H, Deng YL, et al. Comparative epidemiological investigation of Alzheimer’s disease and colorectal cancer: the possible role of gastrointestinal conditions in the pathogenesis of AD. Front Aging Neurosci 2018;10:176.ArticlePubMedPMC
- 28. Tolea MI, Morris JC, Galvin JE. Longitudinal associations between physical and cognitive performance among community-dwelling older adults. PLoS One 2015;10:e0122878.ArticlePubMedPMC
- 29. Pedersen MM, Holt NE, Grande L, Kurlinski LA, Beauchamp MK, Kiely DK, et al. Mild cognitive impairment status and mobility performance: an analysis from the Boston RISE study. J Gerontol A Biol Sci Med Sci 2014;69:1511-1518.ArticlePubMedPMC
- 30. Downer B, Chen NW, Raji M, Markides KS. A longitudinal study of cognitive trajectories in Mexican Americans age 75 and older. Int J Geriatr Psychiatry 2017;32:1122-1130.ArticlePubMedPMCPDF
- 31. Han L, Gill TM, Jones BL, Allore HG. Cognitive aging trajectories and burdens of disability, hospitalization and nursing home admission among community-living older persons. J Gerontol A Biol Sci Med Sci 2016;71:766-771.ArticlePubMedPMC
- 32. Kim G, Choi S, Lyu J. Body mass index and trajectories of cognitive decline among older Korean adults. Aging Ment Health 2020;24:758-764.ArticlePubMed
- 33. McCarrey AC, An Y, Kitner-Triolo MH, Ferrucci L, Resnick SM. Sex differences in cognitive trajectories in clinically normal older adults. Psychol Aging 2016;31:166-175.ArticlePubMedPMC
- 34. Proust-Lima C, Amieva H, Dartigues JF, Jacqmin-Gadda H. Sensitivity of four psychometric tests to measure cognitive changes in brain aging-population-based studies. Am J Epidemiol 2007;165:344-350.ArticlePubMedPMC
- 35. Finkel D, Reynolds CA, Berg S, Pedersen NL. Surprising lack of sex differences in normal cognitive aging in twins. Int J Aging Hum Dev 2006;62:335-357.ArticlePubMedPDF
- 36. Ferreira L, Ferreira Santos-Galduróz R, Ferri CP, Fernandes Galduróz JC. Rate of cognitive decline in relation to sex after 60 yearsof-age: a systematic review. Geriatr Gerontol Int 2014;14:23-31.Article
- 37. Inzitari M, Baldereschi M, Di Carlo A, Di Bari M, Marchionni N, Scafato E, et al. Impaired attention predicts motor performance decline in older community-dwellers with normal baseline mobility: results from the Italian Longitudinal Study on Aging (ILSA). J Gerontol A Biol Sci Med Sci 2007;62:837-843.ArticlePubMed
- 38. Alfaro-Acha A, Al Snih S, Raji MA, Markides KS, Ottenbacher KJ. Does 8-foot walk time predict cognitive decline in older Mexicans Americans? J Am Geriatr Soc 2007;55:245-251.ArticlePubMed
- 39. Verghese J, Wang C, Lipton RB, Holtzer R, Xue X. Quantitative gait dysfunction and risk of cognitive decline and dementia. J Neurol Neurosurg Psychiatry 2007;78:929-935.ArticlePubMedPMC
- 40. Atkinson HH, Cesari M, Kritchevsky SB, Penninx BW, Fried LP, Guralnik JM, et al. Predictors of combined cognitive and physical decline. J Am Geriatr Soc 2005;53:1197-202.ArticlePubMed
- 41. Pedersen BK, Febbraio M. Muscle-derived interleukin-6--a possible link between skeletal muscle, adipose tissue, liver, and brain. Brain Behav Immun 2005;19:371-376.ArticlePubMed
- 42. Xu H, Dupre ME, Gu D, Wu B. The impact of residential status on cognitive decline among older adults in China: results from a longitudinal study. BMC Geriatr 2017;17:107.ArticlePubMedPMCPDF
- 43. Tang HD, Zhou Y, Gao X, Liang L, Hou MM, Qiao Y, et al. Prevalence and risk factor of cognitive impairment were different between urban and rural population: a community-based study. J Alzheimers Dis 2016;49:917-925.ArticlePubMed
- 44. Saenz JL, Downer B, Garcia MA, Wong R. Cognition and context: rural-urban differences in cognitive aging among older Mexican adults. J Aging Health 2018;30:965-986.ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
- Mediation role of DNA methylation in association between handgrip strength and cognitive function in monozygotic twins
Jin Liu, Weijing Wang, Jia Luo, Haiping Duan, Chunsheng Xu, Xiaocao Tian, Shumin Chen, Lin Ge, Dongfeng Zhang
Journal of Human Genetics.2024;[Epub] CrossRef - Longitudinal trajectories of cognitive aging
Elena Lobo, Patricia Gracia-García, Antonio Lobo
Current Opinion in Psychiatry.2023;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite