
Articles
- Page Path
- HOME > Epidemiol Health > Volume 45; 2023 > Article
-
Original Article
Changes in the treatment rate of patients newly diagnosed with stage IV cancer near the end of life from 2012 to 2017 in Korea -
Kyuwoong Kim1
 , Hyun Jung Jho1,2, So Jung Park1,2, Bohyun Park1, Jin Young Choi1
, Hyun Jung Jho1,2, So Jung Park1,2, Bohyun Park1, Jin Young Choi1 -
Epidemiol Health 2023;45:e2023021.
DOI: https://doi.org/10.4178/epih.e2023021
Published online: February 14, 2023
1National Hospice Center, National Cancer Control Institute, Goyang, Korea
2Department of Hospice Palliative Service, National Cancer Center, Goyang, Korea
- Correspondence: Jin Young Choi National Hospice Center, National Cancer Control Institute, 323 Ilsan-ro, Ilsandong-gu, Goyang 10408, Korea E-mail: ilotopie@ncc.re.kr
© 2023, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,864 Views
- 154 Download
Abstract
-
OBJECTIVES
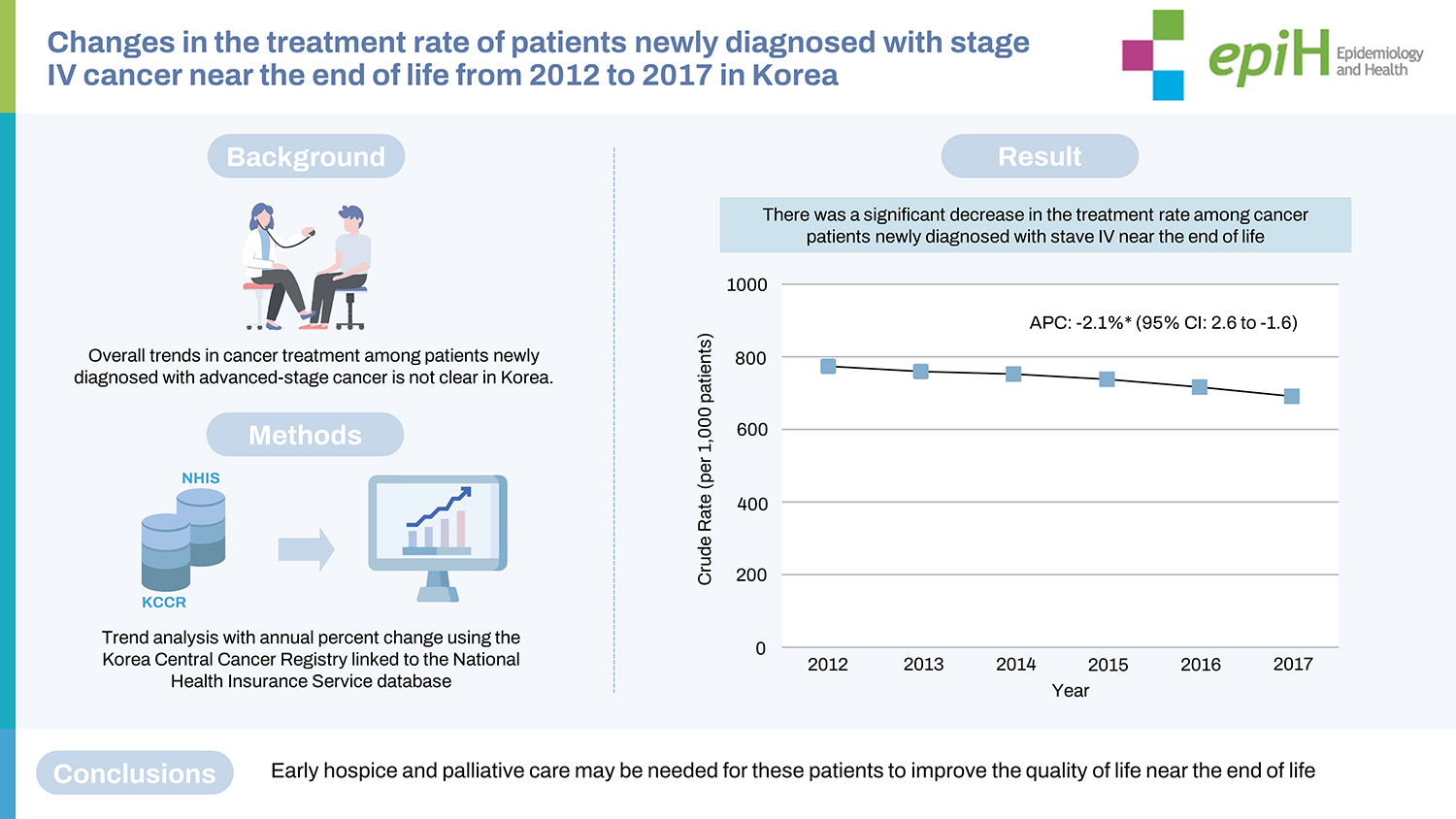
- This study aimed to evaluate changes in the cancer treatment rate among patients newly diagnosed with stage IV cancer using socio-demographic and clinical subgroups in a nationwide cohort of Korean patients.
-
METHODS
- This retrospective, national-level study used the Korea Central Cancer Registry (KCCR), which is linked to the National Health Insurance Service (NHIS) database, from January 1, 2012 to December 31, 2017. The records of patients newly diagnosed with stage IV of the 5 cancers with the highest cancer-related mortality rate were identified to analyze changes in the treatment rate. The main outcome examined in this study was the change in the cancer treatment rate between 2012 and 2017, as measured using the annual percent change (APC).
-
RESULTS
- A total of 106,082 patients with newly diagnosed gastric, colorectal, liver, pancreatic, and lung cancers at the end of life (EoL) were identified from the KCCR-NHIS database. Of these patients, 76,533 (72.1%) received cancer treatment. Over the study period (2012-2017), the proportion of patients who received cancer treatment at EoL decreased by 8.3%, with an APC of -2.1% (95% confidence interval, -2.6 to -1.6). This declining trend of cancer treatment among patients with advanced cancer stage at EoL was consistent among socio-demographic and clinical subgroups.
-
CONCLUSIONS
- The proportion of untreated patients with stage IV cancer is increasing in the Korea. For patients who are not undergoing standard cancer treatment near EoL, an alternative care plan, such as early palliative care, should be considered.
- Cancer, followed by cardiovascular disease, is the leading cause of mortality worldwide, resulting in approximately 10 million deaths in 2020 [1]. In the recent analysis of the Prospective Urban Rural Epidemiology study, hospital admission and death rates from cancer in high-income countries were nearly 2-fold to 3-fold higher than those in middle-income and low-income countries across 5 continents [2]. Based on current trends in cancer incidence and mortality, the global burden of cancer is expected to double by 2070 if additional cancer control plans are not implemented worldwide [3]. Despite the use of traditional and newly emerging health-related risk factors [4-11], the cancer stage at diagnosis continues to be a strong predictor of cancer mortality [12-14].
- Most randomized controlled trials and observational studies have demonstrated improved survival outcomes among patients with advanced cancer stage who received conventional or novel treatments compared to those who did not [15,16], but these studies have not extensively addressed those who were not treated for cancer near the end of life (EoL) [17]. Currently, there is a paucity of data on overall trends of cancer treatment among patients newly diagnosed with advanced-stage cancer near EoL, which is a proxy for the accessibility of standard or alternative cancer care, including hospice and palliative care (HPC) services [18-20]. Generally, the main needs of cancer patients at their EoL are multifactorial, ranging from psychiatric care to social support from clinicians and caregivers [21,22]. Moreover, even though aggressive treatment for patients with advanced cancer is relatively affordable under a single-payer healthcare system in Korea compared to privatized healthcare systems elsewhere, there are limited data on recent trends in the treatment rate and its differences between socio-demographic and clinical subgroups [23,24].
- This study aimed to compare up-to-date, large-scale, administrative data on the aforementioned trends among patients with stage IV cancer near their EoL in Korea between socio-demographic and clinical subgroups to evaluate whether treatment trends are changing.
INTRODUCTION
- Study design
- We conducted a population-based, retrospective cohort study using nationwide data from the Korea Central Cancer Registry linked to the National Health Insurance Service (KCCR-NHIS) from January 1, 2012 to December 31, 2017 to investigate trends in cancer treatment near EoL by cancer types, socio-demographic factors, and clinical characteristics. We also evaluated trends in types of cancer treatment among patients who received treatment.
- Data source
- We collected data on the 5 non-sex-specific cancers with the highest cancer-related mortality rates from the KCCR, which is a nationwide cancer registry that is extensively used for monitoring cancer incidence, mortality, and survival and was established by the Ministry of Health and Welfare and operated by the National Cancer Center in Korea. After identifying newly diagnosed cases of stage IV gastric, colorectal, liver, pancreatic, and lung cancers using the Surveillance, Epidemiology, and End Results Program (SEER) staging guidelines in KCCR, we linked the data of these patients to the NHIS to obtain information on the socio-demographic factors and clinical characteristics from the insurance eligibility and medical claims records of the NHIS, respectively. Briefly, the NHIS is the single insurer for health insurance in Korea, with a coverage rate of approximately 97%. The NHIS provides a variety of databases, including those for insurance premiums, which serve as a proxy for income status, and pharmaceutical prescription claims, for research purposes, especially for epidemiological studies and health policymaking. The details of the KCCR and NHIS databases have been described in previous studies [25-27].
- Population
- The study population included adult patients aged ≥ 20 years enrolled in the database between 2012 and 2017 with records of newly diagnosed stage IV gastric, colorectal, liver, pancreas, or lung cancers, which are the leading causes of cancer-related mortality for both male and female in Korea [26]. Cancer types in the KCCR database were identified using the International Classification of Diseases for Oncology, 3rd edition. We excluded patients with cancers identified in the medical claims records in any site prior to the diagnosis year according to the International Classification of Diseases, 10th revision (C00-C97). To explore treatment trends near EoL, we only included patients who died within 2 years after the initial diagnosis (n= 106,082). The selection criteria for the study population are shown in Figure 1.
- Measures
- Cancer treatment was measured using the NHIS records pertaining to medical claims for monotherapy (surgery only, chemotherapy only, and radiation therapy only) and combination therapy (2 or more therapies). We retrieved the medical claims records for cancer treatment from the initial diagnosis to death among the patients enrolled. For the primary outcome, patients treated for cancer were defined as those who had received any type of treatment during the study period, whereas those who had no treatment were defined as untreated. Socio-demographic and clinical variables included age (< 70 and ≥ 70 years of age considered to indicate non-elderly and elderly status, respectively), sex (male or female), place of residence (categorized with administrative codes as capital, metropolitan, or rural), insurance type (employee insured or self-employed insured), insurance premium (grouped into quartile representing income status), and Charlson comorbidity index (CCI, calculated from the medical claims records prior to the first-ever cancer diagnosis).
- Statistical analysis
- The socio-demographic and clinical characteristics of treated and untreated patients are presented as numbers and percentages for each variable. The chi-square test was used to compute p-values between the 2 aforementioned populations for each characteristic. To assess the yearly treatment rate, we computed the proportion of patients who were treated for stage IV cancer as the crude rate (CR) per 1,000 patients. We also calculated the CR per 1,000 people for the treatment and non-treatment rates as stratified according to cancer sites (gastric, colorectal, liver, pancreas, and lung) and socio-demographic (age, sex, place of residence, insurance type, and insurance premium) and clinical characteristics (CCI). Among the treated patients, the crude proportions for types of treatment near EoL were calculated. To estimate the changing trends in these treatment patterns from 2012 to 2017, we computed annual percent changes (APCs) with 95% confidence intervals (CIs).
- As a sensitivity analysis, we additionally computed APCs with 95% CIs for the cancer treatment rate derived from the age-standardized rate (ASR) using the population aged more than 20 years in 2012 as the standard population. Statistical significance was 2-sided, and a p-value < 0.05 was considered statistically significant. Data collection and analyses of patient characteristics and treatment patterns each year were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The Joinpoint Regression Program version 4.9.0.1 from the National Cancer Institute (Rockville, MD, USA) was used to calculate APCs and their 95% CIs for the trend analysis.
- Ethics statement
- This study was approved by the Institutional Review Board of the National Cancer Center (approval No. NCC2020-0064). There was no requirement to obtain verbal or written consent from patients because the KCCR-NHIS database is anonymized according to the Personal Information Protection Act.
MATERIALS AND METHODS
- Study population
- In total, we identified 106,082 patients newly diagnosed with stage IV cancer near EoL from 2012 to 2017, among whom 76,533 (72.1%) were treated and 29,549 (27.9%) were untreated following the diagnosis. Most untreated patients were adults aged ≥ 70 years (71.9%), whereas the proportion of older adults was significantly lower among treated patients than among untreated patients (43.1%). Compared with untreated patients, treated patients more frequently resided in the capital city or a metropolitan area. Lung cancer was the most common type of cancer in both groups (45.4 and 40.6% in the treated and untreated groups, respectively). Among treated patients, chemotherapy alone (57.8%) and combination therapy (37.2%) were the most prevalent types of cancer treatment. Table 1 shows the differences in the socio-demographic and clinical characteristics between treated and untreated patients.
- Trends in cancer treatment near end of life
- Figure 2A shows the CR per 1,000 patients for the trend in cancer treatment in patients newly diagnosed with stage IV cancer near EoL. In 2012, 13,763 (77.7%) patients were treated (CR, 777.6; 95% CI, 764.5 to 790.6), but this proportion decreased by 8.3% in 2017 (CR, 694.8; 95% CI, 681.3 to 708.2). From 2012 to 2017, cancer treatment among these patients significantly decreased, with an APC of -2.1% (95% CI, -2.6 to -1.6; p< 0.05). Figure 2B shows trends in the types of cancer treatment among patients who were treated with either monotherapy or combination therapy. In 2012, 5,498 of 13,763 (39.9%) patients received combination therapy, but this proportion significantly decreased by 8.6% in 2017 with an APC of -4.4% (95% CI, -6.8 to -1.9; p< 0.05). Meanwhile, the proportion of those who received chemotherapy alone significantly increased from 2012 to 2017 (APC, 2.5%; 95% CI, 1.0 to 4.0; p< 0.05). Details of the cancer treatment in each year between 2012 and 2017 are presented in Supplementary Materials 1 and 2. The sensitivity analysis showed that the decreasing trend in cancer treatment remained consistent when the CR was converted to the ASR (APC, -3.4%; 95% CI, -4.5 to -2.3; p< 0.05) (Supplementary Material 3).
- Discrepancies in treatment trend near end of life between cancer sites
- Figure 3 shows the site-specific rates for cancer treatment near EoL among the cancers with the highest cancer-related mortality rates in male and female from 2012 to 2017. The magnitude of the decreasing trend in the cancer treatment rate was the highest among patients with colorectal cancer (APC, -3.4%; 95% CI, -5.7 to -1.1; p< 0.05), followed by those with lung cancer (APC, -2.4%; 95% CI, -2.6 to -2.1; p< 0.05). The APCs for cancer treatment in other sites also showed significantly decreasing trends in patients with gastric cancer (APC, -1.9%; 95% CI, -2.7 to -1.2; p< 0.05) and liver cancer (APC, -1.3%; 95% CI, -2.0 to -0.6; p< 0.05), but a non-significant trend was found in patients with pancreatic cancer (APC, -1.2%; 95% CI, -2.4 to 0.0; p< 0.05). Supplementary Material 4 shows the details on treatment trends by cancer sites between 2012 and 2017.
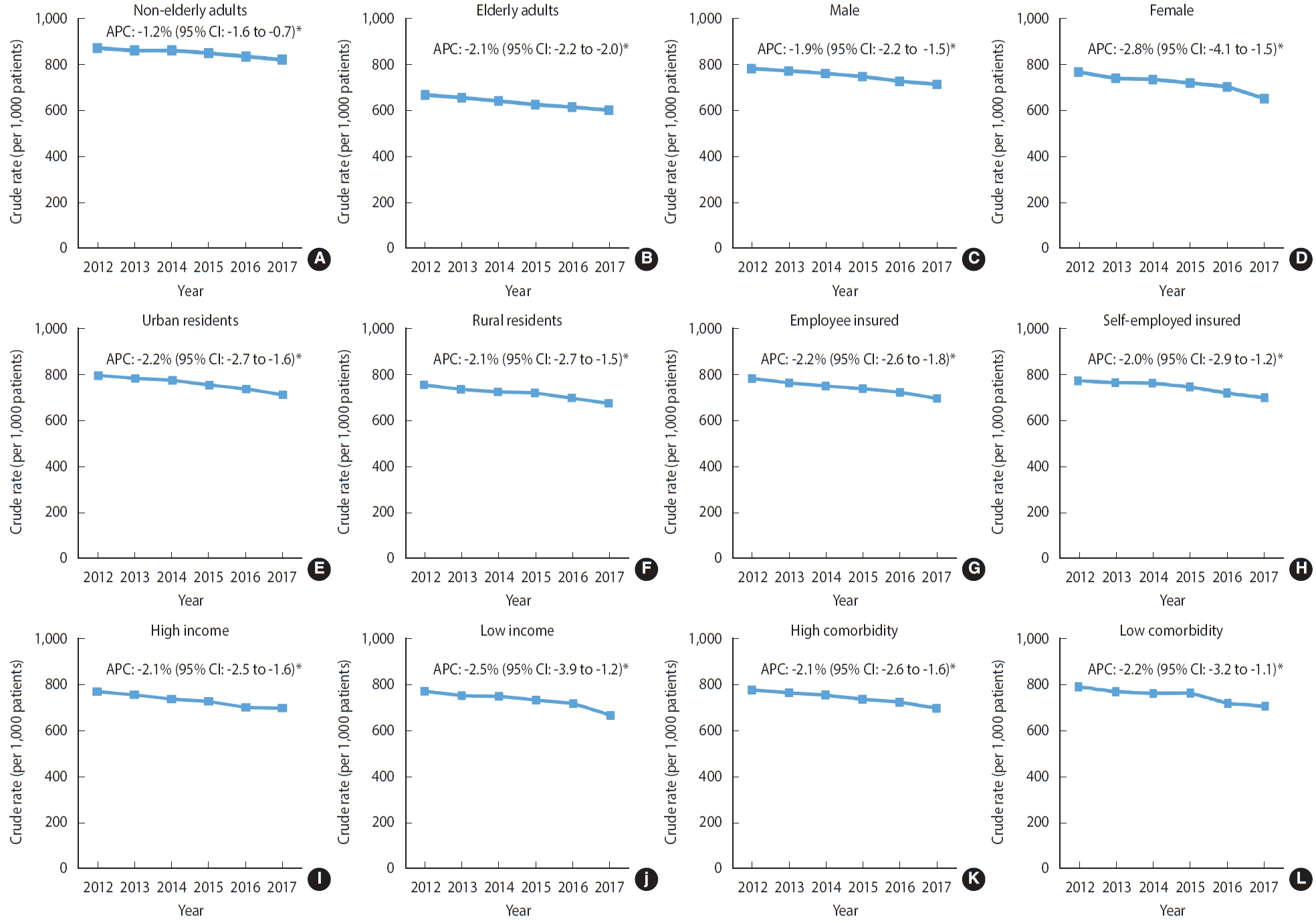
- Treatment trends by socio-demographic and clinical characteristics
- As shown in Figure 4, the decreasing trend in the cancer treatment rate was similar across all socio-demographic and clinical characteristics from 2012 to 2017. Patients aged ≥ 70 years showed a more drastic decrease in the cancer treatment rate (APC, -2.1%; 95% CI, -2.2 to -2.0; p< 0.05) than did those aged ≤ 70 years (APC, -1.2%; 95% CI, -1.6 to -0.7; p< 0.05). Compared with male patients (APC, -1.9%; 95% CI, -2.2 to -1.5; p< 0.05), female patients showed a steeper decline in the rate of cancer treatment over the time period (APC, -2.8%; 95% CI, -4.1 to -1.5; p< 0.05). Decreasing trends of similar magnitude were observed among patients with different residential areas, insurance type, insurance premiums (indicator for income status), and comorbid conditions. Supplementary Material 5 lists the proportions and CRs (95% CI) of treated and untreated patients by their characteristics each year between 2012 and 2017.
RESULTS
- Among the 106,082 patients who were newly diagnosed with stage IV cancers from 2012 to 2017 near EoL in Korea, the rate of cancer treatment showed a progressive decline, most notably among patients with colorectal and lung cancers. Overall, the decreasing trend in cancer treatment was consistent in patients with different socio-demographic and clinical characteristics. Nonetheless, the proportion of patients who were treated for stage IV cancer was persistently around 70% during the study period, representing that most patients near their EoL were still being treated.
- Moreover, the rate of combination therapy declined, and that of chemotherapy alone increased among treated patients throughout the study period. Among those who remained untreated for stage IV cancer near their EoL, the awareness of an alternative clinical approach, such as HPC, and socioeconomic barriers to access to treatment might have partially contributed to the declining trend in the treatment rate.
- Comparison to other studies
- Few studies have measured changes in treatment patterns and clinical outcomes among patients with cancer, but the results were mixed, and those studies have seldom focused on the comprehensive assessment of the treatment rate among stage IV patients near their EoL over time. Data from the Rotterdam Cancer Registry, which holds information on patients in the southwestern part of the Netherlands, showed a 38% and 6% increase in chemotherapy use and hepatic surgery, respectively, among 3,482 patients diagnosed with stage IV colorectal cancer during the study period (1995-2007) [28]. Similar to the Rotterdam study, our findings also show an increasing trend in the use of chemotherapy for cancer treatment between 2012 and 2017 among patients who were treated for stage IV cancers. However, the Rotterdam study only examined the trend in standard oncology treatment, including surgery and chemotherapy, in patients with advanced-stage colorectal cancer, without considering alternative care options, such as the early utilization of HPC. Furthermore, the Rotterdam study was based on a single Dutch city and did not examine patients with stage IV cancer near their EoL. Considering the substantially high treatment rate and improved survival outcomes reported in the Rotterdam study, patients were more likely to cope with treatment compared to those who were clinically unfit to receive treatment due to overall health or degree of cancer progression.
- Consistent with the Rotterdam study, another population-based study conducted among elderly Dutch patients with stage III colon cancer from the Eindhoven Cancer Registry showed an increasing rate of adjuvant chemotherapy between 1995 and 2001 [29]. However, in the Eindhoven study, elderly patients who were female and with low socioeconomic status (SES) and comorbid conditions were less likely to receive this treatment over the study period. In contrast to the Eindhoven study, the results from the current KCCR-NHIS study showed a consistently declining trend in the treatment rate, regardless of SES, including income status and health insurance type, and comorbidities, including the CCI. Moreover, the Eindhoven study used postal codes to estimate SES among elderly patients, rather than directly assessing income or the financial assets of patients. Since SES plays a key role in access to cancer treatment, obtaining accurate measures of SES is critical when examining the changes in cancer treatment trends by socio-demographic subgroups.
- Moreover, the differences in the trend of cancer treatment rate among patients with low SES between the Eindhoven study and current KCCR-NHIS study could be partially explained by the enhanced insurance coverage for cancer treatment under a single insurer system with the NHIS in Korea.
- Study implications
- The findings of this nationwide cohort study have important implications for public health policy for the management of patients with cancer near their EoL, suggesting that patients and their caregivers should be thoroughly informed about available clinical decisions and expected outcomes for each option. In a non-blinded, randomized, controlled trial of patients newly diagnosed with metastatic non-small-cell lung cancer (NSCLC) in the United States, patients with NSCLC who received early utilization of palliative care had improved quality of life (QoL) and better mood and received less aggressive care, including chemotherapy, within 2 weeks prior to death and without hospice care or admission to the hospice ward 3 days or less prior to death, compared to those who received standard cancer care towards their EoL [30].
- Moreover, a recent cost-utility analysis conducted in China suggested that palliative care improved the QoL at EoL and mitigated the economic burden for Chinese patients with advanced cancer [24]. Integrating the evidence from these studies, early HPC, as well as standard oncology care, should be suggested as a viable option for patients whose cancer is unlikely to be cured or successfully managed owing to its advantages. Thus, healthcare professionals and health policymakers should be aware of the potential advantages and disadvantages of both standard oncology care and HPC. Future investigations are warranted to explore whether the decreasing trend of cancer treatment among patients at their EoL is partially attributable to discrepancies in socioeconomic and clinical background among patients, changes in treatment guidelines and health insurance coverage, regional variations in cancer treatment hospitals, and patients’ refusal of life-sustaining treatment.
- Strengths and limitations
- To the best of our knowledge, no previous studies have extensively examined recent trends in the treatment rate of patients with stage IV cancers near their EoL by socio-demographic and clinical subgroups using large-scale observational data in Korea, where the NHIS is the single insurer. In fact, most previous studies have focused on patterns of care and survival outcomes of patients with stage IV or earlier stages. Furthermore, this study was conducted with high-quality data on cancer type, diagnosis date, and SEER stage linked to population-based data on the socio-demographic and clinical situation of patients. Therefore, a major strength of our study is that we abstracted information from the nationwide data on cancer patients near their EoL with a high coverage rate in Korea. In this regard, our study is less prone to selection bias than single-center studies assessing a registry with a low coverage rate. Nevertheless, this study has a few limitations. There was no detailed information on the types of chemotherapy, including direct DNA-interacting agents, targeted therapy, immunotherapy, hormone therapy, and so on, in our dataset. Future studies should assess trends in chemotherapy use among cancer patients at EoL, taking into account differences in the level of toxicity by types of chemotherapy. Moreover, the data obtained from the KCCR-NHIS database do not contain information on the reason behind the decision not to be treated for stage IV cancer, which would include, for example, a high financial burden pertaining to cancer treatment or a desire not to receive aggressive treatment near EoL. However, almost the entire Korean population is enrolled in the NHIS, and those diagnosed with cancer benefit from a substantially discounted copayment rate after the implementation of the health insurance coverage expansion policy for cancer in 2013. Moreover, our study showed a declining treatment rate for both high-income and low-income patients with stage IV cancers. Thus, it is relatively unlikely that the declining trend of cancer treatment near EoL is attributable to cancer-related financial burdens.
- In conclusion, in this nationwide cohort study of KCCR-NHIS data from 2012 to 2017, there was a significantly decreasing trend in the treatment rate of patients diagnosed with stage IV cancers near their EoL, though most patients still received cancer treatment. On the basis of the currently available evidence, alternative clinical choices, such as the early utilization of HPC, may thoroughly improve QoL and reduce aggressive care for patients with advanced-stage cancer at EoL.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
Supplementary Material 4.
Supplementary Material 5.
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This study was supported by the National Cancer Center of the Republic of Korea (grant No. 2010710-2 and 2211830-1).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Kim K, Choi JY. Data curation: Kim K, Park B. Formal analysis: Kim K. Funding acquisition: Choi JY. Methodology: Kim K, Park SJ. Project administration: Choi JY, Jho HJ. Visualization: Park B, Park SJ, Kim K. Writing – original draft: Kim K. Writing – review & editing: Kim K, Jho HJ, Park SJ, Park B, Choi JY.
NOTES
ACKNOWLEDGEMENTS



| Characteristics |
Patients newly diagnosed with stage IV cancer1 |
||||
|---|---|---|---|---|---|
| Treated (n=76,533)2 | Untreated (n=29,549)3 | p-value4 | |||
| Age (yr)5 | |||||
| 20-29 | 210 (0.3) | 21 (0.1) | <0.001 | ||
| 30-39 | 1,576 (2.1) | 193 (0.7) | |||
| 40-49 | 5,581 (7.3) | 821 (3.1) | |||
| 50-59 | 15,164 (19.8) | 2,466 (9.3) | |||
| 60-69 | 21,022 (27.5) | 3,962 (14.9) | |||
| ≥70 | 32,980 (43.1) | 19,086 (71.9) | |||
| Sex | |||||
| Male | 52,788 (69.0) | 17,449 (65.7) | <0.001 | ||
| Female | 23,745 (31.0) | 9,100 (34.3) | |||
| Place of residence | |||||
| Capital city | 14,164 (18.5) | 3,981 (15.0) | <0.001 | ||
| Metropolitan | 33,879 (44.3) | 11,281 (42.5) | |||
| Rural (city/town) | 28,490 (37.2) | 11,287 (42.5) | |||
| Insurance type | |||||
| Employee insured | 49,933 (65.2) | 17,523 (66.0) | 0.026 | ||
| Self-employed insured | 26,600 (34.8) | 9,026 (34.0) | |||
| Insurance premium6 | |||||
| Quartile 1 | 14,854 (19.4) | 5,478 (20.6) | <0.001 | ||
| Quartile 2 | 14,850 (19.4) | 4,726 (17.8) | |||
| Quartile 3 | 18,655 (24.4) | 5,915 (22.3) | |||
| Quartile 4 | 28,174 (36.8) | 10,430 (39.3) | |||
| Cancer type | |||||
| Gastric | 11,875 (15.5) | 3,890 (14.7) | <0.001 | ||
| Colorectal | 11,950 (15.6) | 4,369 (16.5) | |||
| Liver | 7,911 (10.3) | 3,982 (15.0) | |||
| Pancreas | 10,051 (13.1) | 3,540 (13.3) | |||
| Lung | 34,746 (45.4) | 10,768 (40.6) | |||
| Treatment for cancer | |||||
| Monotherapy | |||||
| Surgery | 1,599 (2.1) | - | |||
| Chemotherapy | 44,222 (57.8) | - | |||
| Radiation therapy | 2,250 (2.9) | - | |||
| Combination therapy | 28,462 (37.2) | - | |||
| Charlson comorbidity index7 | |||||
| 0 | 4,900 (6.4) | 1,776 (6.7) | <0.001 | ||
| 1 | 13,144 (17.2) | 4,095 (15.4) | |||
| ≥2 | 58,489 (76.4) | 20,678 (77.9) | |||
Values are presented as number (%).
1 Five non-sex-specific cancers with the highest cancer mortality based on the KCCR report.
2 Patients newly diagnosed with stage IV cancer who underwent surgery, chemotherapy, radiotherapy, or combination treatment prior to death.
3 Patients newly diagnosed with stage IV cancer who did not receive any type of treatment for cancer prior to death.
4 Computed with the chi-square test.
5 Age at the time of first-ever stage IV cancer diagnosis.
6 Proxy for individual-level income status.
7 Without accounting for assigned weights in comorbid conditions related to cancer.
- 1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209-249.ArticlePubMedPDF
- 2. Dagenais GR, Leong DP, Rangarajan S, Lanas F, Lopez-Jaramillo P, Gupta R, et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study. Lancet 2020;395:785-794.ArticlePubMed
- 3. Soerjomataram I, Bray F. Planning for tomorrow: global cancer incidence and the role of prevention 2020-2070. Nat Rev Clin Oncol 2021;18:663-672.ArticlePubMedPDF
- 4. Ekelund U, Brown WJ, Steene-Johannessen J, Fagerland MW, Owen N, Powell KE, et al. Do the associations of sedentary behaviour with cardiovascular disease mortality and cancer mortality differ by physical activity level? A systematic review and harmonised meta-analysis of data from 850 060 participants. Br J Sports Med 2019;53:886-894.ArticlePubMed
- 5. Harper S, Lynch J, Meersman SC, Breen N, Davis WW, Reichman MC. Trends in area-socioeconomic and race-ethnic disparities in breast cancer incidence, stage at diagnosis, screening, mortality, and survival among women ages 50 years and over (1987-2005). Cancer Epidemiol Biomarkers Prev 2009;18:121-131.ArticlePubMedPDF
- 6. Ries LA, Young JL, Keel GE, Eisner MP, Lin YD, Horner MJ. Cancer survival among adults: U.S. SEER program, 1988-2001: patient and tumor characteristics; 2007 [cited 2022 Dec 28]. Available from: https://seer.cancer.gov/archive/publications/survival/seer_survival_mono_highres.pdf.
- 7. Falchook AD, Dusetzina SB, Tian F, Basak R, Selvam N, Chen RC. Aggressive end-of-life care for metastatic cancer patients younger than age 65 years. J Natl Cancer Inst 2017;109:djx028.ArticlePubMedPMC
- 8. Greer JA, Jackson VA, Meier DE, Temel JS. Early integration of palliative care services with standard oncology care for patients with advanced cancer. CA Cancer J Clin 2013;63:349-363.ArticlePubMed
- 9. Shalev A, Phongtankuel V, Kozlov E, Shen MJ, Adelman RD, Reid MC. Awareness and misperceptions of hospice and palliative care: a population-based survey study. Am J Hosp Palliat Care 2018;35:431-439.ArticlePubMedPMCPDF
- 10. Clayton JM, Butow PN, Tattersall MH. The needs of terminally ill cancer patients versus those of caregivers for information regarding prognosis and end-of-life issues. Cancer 2005;103:1957-1964.ArticlePubMed
- 11. Yoo KY. Cancer control activities in the Republic of Korea. Jpn J Clin Oncol 2008;38:327-333.ArticlePubMed
- 12. Biagi JJ, Raphael MJ, Mackillop WJ, Kong W, King WD, Booth CM. Association between time to initiation of adjuvant chemotherapy and survival in colorectal cancer: a systematic review and meta-analysis. JAMA 2011;305:2335-2342.ArticlePubMed
- 13. Connor SR. Development of hospice and palliative care in the United States. Omega (Westport) 2007- 2008;56:89-99.ArticlePDF
- 14. van der Pool AE, Damhuis RA, Ijzermans JN, de Wilt JH, Eggermont AM, Kranse R, et al. Trends in incidence, treatment and survival of patients with stage IV colorectal cancer: a population-based series. Colorectal Dis 2012;14:56-61.ArticlePubMed
- 15. David EA, Daly ME, Li CS, Chiu CL, Cooke DT, Brown LM, et al. Increasing rates of no treatment in advanced-stage non-small cell lung cancer patients: a propensity-matched analysis. J Thorac Oncol 2017;12:437-445.ArticlePubMedPMC
- 16. Clark K. Care at the very end-of-life: dying cancer patients and their chosen family’s needs. Cancers (Basel) 2017;9:11.ArticlePubMedPMC
- 17. McPhail S, Johnson S, Greenberg D, Peake M, Rous B. Stage at diagnosis and early mortality from cancer in England. Br J Cancer 2015;112(Suppl 1):S108-S115.ArticlePubMedPMCPDF
- 18. Ohkuma T, Peters SA, Woodward M. Sex differences in the association between diabetes and cancer: a systematic review and meta-analysis of 121 cohorts including 20 million individuals and one million events. Diabetologia 2018;61:2140-2154.ArticlePubMedPMCPDF
- 19. Walters S, Maringe C, Coleman MP, Peake MD, Butler J, Young N, et al. Lung cancer survival and stage at diagnosis in Australia, Canada, Denmark, Norway, Sweden and the UK: a populationbased study, 2004-2007. Thorax 2013;68:551-564.ArticlePubMed
- 20. Cho DY, Park J, Kim DS. The impact of expanding health insurance coverage for anti-cancer drugs on cancer survival in Korea. Cancer Med 2021;10:4555-4563.ArticlePubMedPMCPDF
- 21. Fiolet T, Srour B, Sellem L, Kesse-Guyot E, Allès B, Méjean C, et al. Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ 2018;360:k322.ArticlePubMedPMC
- 22. Llaha F, Gil-Lespinard M, Unal P, de Villasante I, Castañeda J, Zamora-Ros R. Consumption of sweet beverages and cancer risk. A systematic review and meta-analysis of observational studies. Nutrients 2021;13:516.ArticlePubMedPMC
- 23. Ciabattini M, Rizzello E, Lucaroni F, Palombi L, Boffetta P. Systematic review and meta-analysis of recent high-quality studies on exposure to particulate matter and risk of lung cancer. Environ Res 2021;196:110440.ArticlePubMed
- 24. Wu H, Lin P, Yang S, Zhang W, Tao W. Cost-utility analysis of palliative care in patients with advanced cancer: a retrospective study. BMC Palliat Care 2021;20:126.ArticlePubMedPMCPDF
- 25. Seong SC, Kim YY, Khang YH, Park JH, Kang HJ, Lee H, et al. Data resource profile: the National Health Information Database of the National Health Insurance Service in South Korea. Int J Epidemiol 2017;46:799-800.PubMed
- 26. Hong S, Won YJ, Park YR, Jung KW, Kong HJ, Lee ES, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2017. Cancer Res Treat 2020;52:335-350.ArticlePubMedPMCPDF
- 27. Jung KW, Won YJ, Kong HJ, Lee ES. Prediction of cancer incidence and mortality in Korea, 2019. Cancer Res Treat 2019;51:431-437.ArticlePubMedPMCPDF
- 28. van der Pool AE, Damhuis RA, Ijzermans JN, de Wilt JH, Eggermont AM, Kranse R, et al. Trends in incidence, treatment and survival of patients with stage IV colorectal cancer: a populationbased series. Colorectal Dis 2012;14:56-61.ArticlePubMed
- 29. van Steenbergen LN, Lemmens VE, Rutten HJ, Wymenga AN, Nortier JW, Janssen-Heijnen ML. Increased adjuvant treatment and improved survival in elderly stage III colon cancer patients in The Netherlands. Ann Oncol 2012;23:2805-2811.ArticlePubMed
- 30. Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 2010;363:733-742.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite





