
Articles
- Page Path
- HOME > Epidemiol Health > Volume 44; 2022 > Article
-
Original Article
Mediation analysis of leisure activities on the association between cognitive function and mortality: a longitudinal study of 42,942 Chinese adults 65 years and older -
Xingxing Chen1,2*
 , Wenfan Wu3*, Xian Zhang2,3, Tingxi Long2, Wenyu Zhu4, Rundong Hu2, Xurui Jin2,3, Lijing L. Yan1,2,5,6, Yao Yao7,8
, Wenfan Wu3*, Xian Zhang2,3, Tingxi Long2, Wenyu Zhu4, Rundong Hu2, Xurui Jin2,3, Lijing L. Yan1,2,5,6, Yao Yao7,8 -
Epidemiol Health 2022;44:e2022112.
DOI: https://doi.org/10.4178/epih.e2022112
Published online: November 27, 2022
1School of Public Health, Wuhan University, Wuhan, China
2Global Health Research Center, Duke Kunshan University, Kunshan, China
3MindRank AI Ltd., Hangzhou, China
4Department of Geriatrics, Affiliated Kunshan Hospital of Jiangsu University, Kunshan, China
5Duke Global Health Institute, Duke University, Durham, NC, USA
6Institute for Global Health and Management, Peking University, Beijing, China
7China Center for Health Development Studies, Peking University, Beijing, China
8Center for Healthy Aging and Development Studies at National School of Development, Peking University, Beijing, China
- Correspondence: Lijing L. Yan, Global Health Research Center, Duke Kunshan University, 8 Duke Avenue, Kunshan 215316, China, E-mail: lijing.yan@duke.edu
- Co-correspondence: Yao Yao, China Center for Health Development Studies, Peking University, 38 Xueyuan Road, Haidian District, Beijing 100191, China, E-mail: yao.yao@bjmu.edu.cn
- * Chen & Wu contributed equally to this work as joint first authors.
© 2022, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
OBJECTIVES
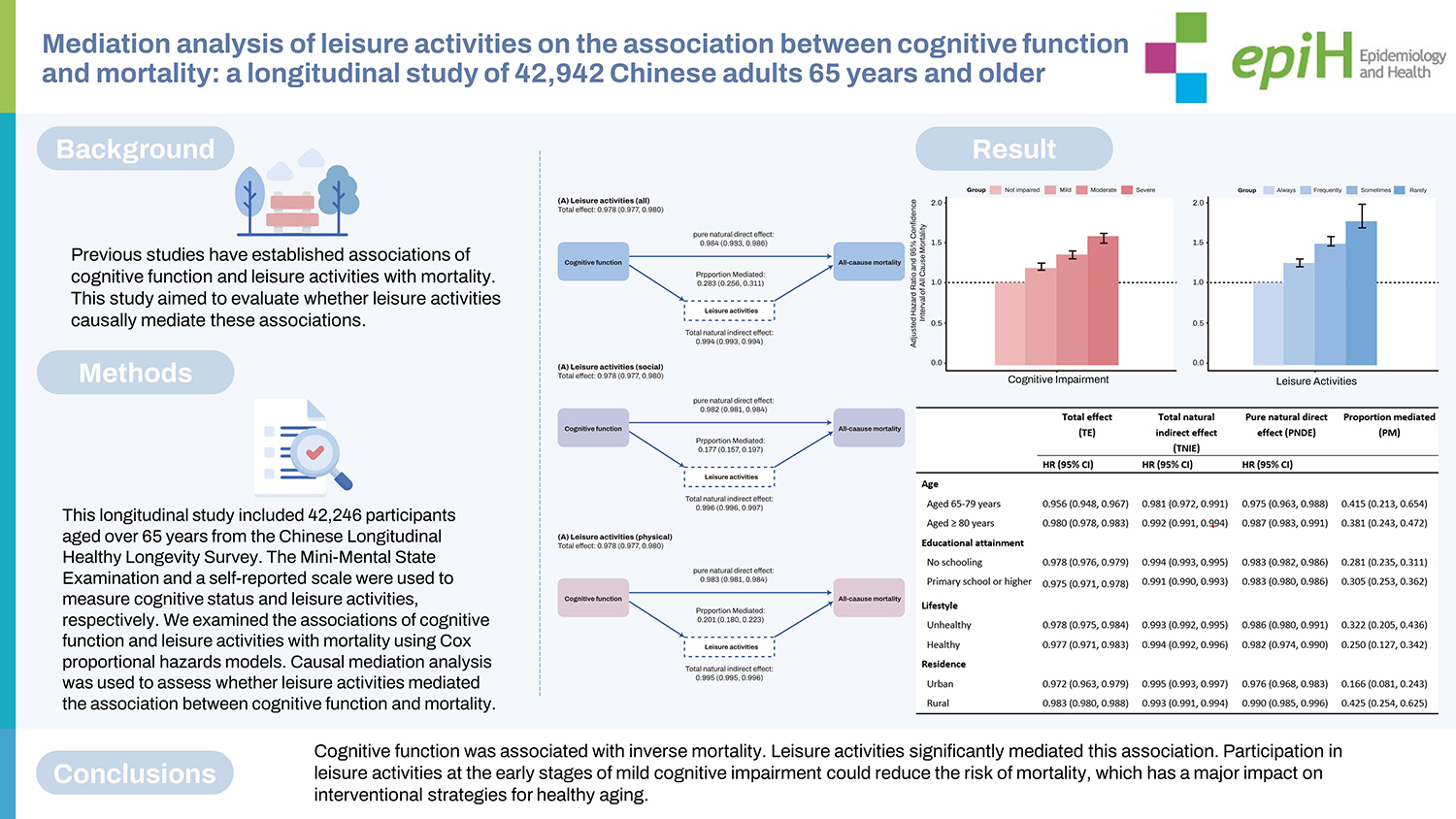
- Previous studies have established associations of cognitive function and leisure activities with mortality. This study aimed to evaluate whether leisure activities causally mediate these associations.
-
METHODS
- This longitudinal study included 42,246 participants aged over 65 years from the Chinese Longitudinal Healthy Longevity Survey. The Mini-Mental State Examination and a self-reported scale were used to measure cognitive status and leisure activities, respectively. We examined the associations of cognitive function and leisure activities with mortality using Cox proportional hazards models. Causal mediation analysis was used to assess whether leisure activities mediated the association between cognitive function and mortality.
-
RESULTS
- Cognitive function and leisure activities were inversely associated with mortality. Leisure activities accounted for 28.3% (95% confidence interval [CI], 25.6 to 31.1) of the total effect of cognitive function and mortality. A higher mediated proportion (PM) was observed for physical leisure activities (PM, 20.1%; 95% CI, 18.0 to 22.3) than for social leisure activities (PM, 17.7%; 95% CI, 15.7 to 19.7). The mediating effect was higher among participants at younger ages (PM, 41.5%; 95% CI, 21.3 to 65.4), those with higher education levels (PM, 30.5%; 95% CI, 25.3 to 36.2), and residents of rural China (PM, 42.5%; 95% CI, 25.4 to 62.5).
-
CONCLUSIONS
- Cognitive function was associated with inverse mortality. Leisure activities significantly mediated this association. Participation in leisure activities at the early stages of mild cognitive impairment could reduce the risk of mortality, which has a major impact on interventional strategies for healthy aging.
- A series of epidemiological studies have demonstrated that lower cognitive function is associated with adverse outcomes such as increased use of home healthcare [1], hospitalization [2], and mortality in older adults [3–6]. However, the mediators of this pathway, through which cognitive impairment increases the mortality rate, remain unclear. The number of people with cognitive impairment is growing with the rapid progress of population aging, resulting in a prioritization of interventions aiming to reduce the risk of mortality due to cognitive impairment.
- Previous studies have shown that cognitive impairment increases the risk of developing neurodegenerative diseases (e.g., stroke or dementia), which in turn is related to higher rates of mortality [7]. However, interventions to delay the progress of neurodegenerative diseases have exhibited poorer performance in reducing the mortality rates among people with cognitive impairment [8]. Accordingly, more studies are needed to study the mediators between cognitive impairment and mortality to provide more evidence for designing such interventions. In a recent observational study, leisure activities demonstrated a greater potential to reduce mortality in older adults with cognitive impairment compared to those who were not cognitively impaired [9]. This finding may indicate that leisure activities could serve as a mechanism for explaining the association between cognitive function and mortality. Even so, there is a lack of evidence relating leisure activities to cognitive function and mortality, particularly those exploring their causal relationship.
- It is difficult to determine whether leisure activities mediate the relationship between cognitive function and mortality statistically. Although the commonly used structural equation modeling method can explore the mediating path by using both cross-sectional data and longitudinal data, it performs poorly when handling survival data. A newly developed longitudinal causal mediation approach may provide a solution [10]. This analysis is based on a counterfactual framework [11], which could be used to clarify the causality between cognitive function and mortality, and to identify potential mediating pathways that provide evidence for interventional study designs.
- We aimed to explore the causal mediating effect of leisure activities on the association between cognitive function and mortality among a nationwide population-based sample of Chinese adults aged 65 years or older. We hypothesized that leisure activities would mediate the association between cognitive function and mortality.
INTRODUCTION
- Study design and participants
- We used data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), which has been conducted since 1998 with follow-ups every 2–3 years. The CLHLS surveys were conducted in randomly selected counties and cities that accounted for half of all counties and cities in 23 out of the 31 provinces of China, covering over 85% of China’s population. The CLHLS sampling frame started with lists of centenarians that are available at the county/city level (lists of adults aged 80+ are not readily available at this level because their population size is too large). Almost all centenarians were interviewed, with few refusals. For every centenarian, the CLHLS interviewed a randomly selected nearby octogenarian and a nearby nonagenarian with a predesignated age and sex. The term “nearby” refers to the same village or street, or the same town, county, or city, where applicable. The goal of the sampling strategy was to include comparable numbers of randomly selected male and female at ages 80 to 99 so that each subsequent wave could have a sufficient number of very old respondents in the sample. Starting in the third wave in 2002, the CLHLS included young-old adults aged 65 to 79 as a comparison group. The sample selection strategy for the young-old adults was the same as that for the oldest-old. As all adults aged 65 to 99 were randomly selected, the CLHLS sample represents older adults in China very well. All data were collected through face-to-face interviews by trained interviewers who were local staff members from the county-level network system of the National Bureau of Statistics of China.
- We pooled 43,487 participants aged 65 years or above at baseline from the 1998 to 2011/2012 waves, with the latest follow-up until 2014 from the CLHLS. To select a group meeting the criteria, we excluded 57 respondents whose age was below 65 and 488 respondents lost to follow-up in the 2014 wave. We also dropped 696 cases with missing information on key variables, leaving a sample of 42,246 for the analysis, which included 16,445 survivors and 25,801 deaths. The details of this survey have been published elsewhere [12]. The follow-up period was up to 16.5 years (median, 3.78), and 61% (n=25,801) of participants died during the follow-up period until 2014. The flow chart of study population is shown in Supplementary Material 1.
- Exposure
- The exposure was cognitive function, which was assessed for all participants using the Chinese version of the Mini-Mental State Examination (MMSE) during each survey through a home-based interview.
- The Chinese MMSE has been proven to be reliable and valid in previous studies [13–15]. The Chinese MMSE consists of 24 components encompassing 7 subdomains: orientation (4 components for time orientation and 1 component for place orientation); naming foods (naming as many kinds of food as possible in 1 minute, one component); registration of 3 words 3 components; attention and calculation (mentally subtracting 3 iteratively from 20, 5 components); copying a figure (1 component); recall (delayed recall of the 3 words mentioned above, 3 components); and language (2 components for naming objectives, 1 component for repeating a sentence, and 3 components for listening and obeying).
- According to the literature [16,17], we classified cognitive impairment into 4 groups (not impaired: 30–25 [MMSE score]; mild: 24–18; moderate: 17–10; severe: 9–0). In our study, we considered responses of “unable to answer” as a “wrong answer” [18,19]. The MMSE score ranged from 0 to 30, with a lower score indicating worse cognitive function.
- Mediator
- Data on self-reported leisure activities were collected through 8 questions to assess the type of leisure activities in which respondents most frequently participated.
- Respondents were asked if they were presently engaged in 8 leisure components, including: (1) housework (cooking or childcare), (2) fieldwork, (3) garden work, (4) reading newspapers/books, (5) raising domestic animals, (6) playing cards and/or mahjong, (7) watching television and/or listening to the radio, and (8) social activities. We then grouped the 8 leisure activities into 2 categories: social leisure activities (housework, playing cards/mahjongg, and social activities), and physical leisure activities (doing fieldwork, gardenwork, reading newspapers/books, watching television/listening to the radio, and raising domestic animals) [20].
- For each leisure component, the frequency was categorized into 3 scores: “almost every day” (scored as 3 points), “sometimes or occasionally” (scored as 2 points), and “rarely or never” (scored as 1 point). Composite scores were calculated for social leisure activities (3 items, ranging from 3 to 9), physical leisure activities (5 items, ranging from 5 to 15), and leisure activities (the sum of all 8 activities, ranging from 8 to 24) separately [21]. The reliability and validity of self-reported leisure activities have been examined in previous research [20].
- Outcome
- Information on vital status and date of death were collected from officially issued death certificates provided by the local government department. When such information was not available, knowledgeable relatives of the decedents were interviewed. The duration of follow-up was calculated by the time interval between the first interview date and the date of death. Participants who survived the last interview were regarded as being censored on the date of their last interview in 2014.
- Covariates
- All covariates included in the present study were categorized into the following 3 groups: demographic characteristics, health behaviors, and disease conditions. Demographic characteristics included age at baseline, sex, education attainment (none, primary school, or middle school or higher), ethnicity (Han vs. minority), place of residence (urban vs. rural), marital status (currently married and living with their spouse, separated/divorced/never married, or widowed), and occupation before 60 years old (manual vs. non-manual). Health behaviors included smoking status (never vs. ever), drinking status (never vs. ever), frequency of drinking tea (every day or occasionally vs. rarely or never), lifestyle (healthy vs. unhealthy) and regular physical activity (yes vs. no). Details on disease conditions were collected through a series of self-reported questions on diseases. The following 8 kinds of self-reported diseases (dichotomized as with vs. without) were included in our study: heart disease, stroke, diabetes, cancer, chronic obstructive pulmonary disease, hypertension, Parkinson’s disease, and bedsore.
- Statistical analysis
- We described the baseline characteristics of the study sample, providing the count and percentage for categorical variables and median and interquartile range for continuous variables. The Kruskal-Wallis H-test for continuous variables and the chi-square test for categorical variables were applied to compare differences by different cognitive function categories. Hazard ratios (HRs) and 95% confidence intervals (CIs) were used to determine the associations between cognitive function, leisure activities, and mortality using Cox proportional-hazard regression models. We tested and ascertained that the proportional-hazard assumption had not been violated.
- A simple conceptual diagram of the current study is shown in Supplementary Material 2. Considering the cognition-related components contained in leisure activities and their features in the causal pathway between cognitive function and mortality, any adjustment for leisure activities as a confounder would render the associations biased [22]. Thus, we undertook a causal mediation analysis based on a counterfactual framework to assess the mediating role of leisure activities in the association between cognitive function and mortality using 3-way decomposition [23,24], which decomposes the total effect (TE) into 3 components. The definitions and interpretations of each of these components in the context of this study are shown in Table 1.
- In order to assess disparities across different populations, we also conducted subgroup analyses by age groups (65–79 vs. ≥80 years), education (no schooling vs. primary or higher), lifestyle (healthy vs. unhealthy), and residence (urban vs. rural), respectively. We also conducted causal mediation analyses for 7 subdomains of cognitive function and mortality.
- We conducted several sensitivity analyses to check the robustness of the results: (1) including participants who had missing values for key variables to examine whether the missing data affected the robustness of the results; (2) excluding participants who died within 2 years after the baseline survey when survival analysis was applied; (3) applying an interaction effect when conducting causal mediation analysis; (4) estimating the controlled direct effect (CDE) across the range of leisure activities score from 8 to 24 to observe a moderating effect.
- The 3-way decomposition was conducted using R (‘regmedint’) [25]. A 2-tailed p-value less than 0.05 was considered statistically significant. All analyses were performed using R version 4.1.1 (R Core Team, Vienna, Austria).
- Ethics statement
- The CLHLS was approved by the Biomedical Ethics Committee of Peking University (IRB00001052-13074) and was conducted in accordance with the guidance of the Declaration of Helsinki.
MATERIALS AND METHODS
- Baseline characteristics
- Table 2 presents the descriptive baseline characteristics of different cognitive function groups. The mean age of participants was 91 years (range, 65–122) and more than half of them (59.1%) were female. The self-reported mean score of leisure activities was 12 (25th and 75th quantiles: 9 and 14). Participants with worse cognitive function (i.e., lower scores on the MMSE) were more likely to be older, female, lower educated, and ethnic Han, to live in rural areas, to be widowed or separated, and to have had manual occupations, lack physical activity, frequently consume tea, have an unhealthy lifestyle, and have lower leisure activity scores (all p<0.001). Participants with worse cognitive function were less likely to smoke and drink (all p<0.001).
- Cognitive function, leisure activities, and mortality
- The multivariate Cox models demonstrated dose–response patterns between cognitive impairment and mortality (Figure 1A). A lower MMSE score was associated with a higher rate of mortality (reference: not impaired, mild: HR, 1.17; 95% CI, 1.14 to 1.22, moderate: HR, 1.32; 95% CI, 1.27 to 1.36, severe: HR, 1.53; 95% CI, 1.45 to 1.56). Leisure activities and mortality showed a consistent dose-response relationship (Figure 1B). Compared with those who participated in leisure activities regularly, those who seldom did so had an increased risk of mortality, with a HR of 1.77 (95% CI, 1.69 to 1.98).
- Causal mediation analysis
- The results of the causal mediation analysis are shown in Figure 2. The TE between cognitive function and mortality had an HR of 0.978 (95% CI, 0.977 to 0.980). The HRs for the pure natural direct effect (PNDE) (direct effect of cognitive function on mortality) and the total natural indirect effect (TNIE) (mediated effect of leisure activities) were 0.984 (95% CI, 0.983 to 0.986) and 0.994 (95% CI, 0.993 to 0.994), respectively. Thus, 28.3% (95% CI, 25.6 to 31.1) of the TE of cognitive function and mortality was associated with leisure activities. A higher mediated proportion (PM) was observed for physical leisure activities (PM, 20.1%; 95% CI, 18.0 to 22.3) than for social leisure activities (PM, 17.7%; 95% CI, 15.7 to 19.7).
- Subgroup analysis
- The causal mediating effect of leisure activities was higher among participants at younger ages (PM, 41.5%; 95% CI, 21.3 to 65.4), those with higher education levels (PM, 30.5%; 95% CI, 25.3 to 36.2), those with an unhealthy lifestyle (PM, 32.2%; 95% CI, 20.5 to 43.6), and residents of rural China (PM, 42.5%; 95% CI, 25.4 to 62.5) (Table 3 and Supplementary Material 3).
- The results of further causal mediation analysis showed that leisure activities causally mediated the associations between 7 subdomains of cognitive function and mortality (all p<0.001) (Supplementary Material 4).
- Sensitivity analysis
- The TE was robust when applying the interaction effect (Supplementary Material 5), while PNDE, TNIE, and PM showed similar patterns to TE, proving the robustness of 3-way decomposition for the causal mediation estimate. For CDE, the results suggested no moderation effect by fixing the leisure activities score in the range of 8–24 (all HR, 0.984, all p<0.001). We included participants who had missing values for key variables and then carried out the causal mediation analysis, and the results showed that the imputed data would not cause bias when estimating the effect (Supplementary Material 6). After excluding participants who died within 2 years after baseline (Supplementary Material 7), the dose-response relationships of both cognitive function and leisure activities with mortality remained consistent.
RESULTS
- We found that cognitive function and leisure activities were negatively associated with mortality in this prospective cohort study of 42,942 Chinese older adults. In the causal mediation analysis, leisure activities were an important mediator of the association between cognitive function and mortality, with indirect effects via leisure activities contributing 28.3% of the TE. Engaging in leisure activities at an early stage of mild cognitive impairment may reduce the risk of mortality.
- This study confirmed the dose-response relationships of cognitive function and leisure activities with mortality in Chinese older adults, in line with another report [26]. Few studies have examined the relationship between cognitive function and mortality in China to date [27,28], but accumulating evidence supports our conclusion that cognitive function is an independent predictor of an increased risk of death in older people [13]. Furthermore, we also provide more evidence on the association between leisure activities and mortality among Chinese older adults, including watching TV or listening to the radio, playing cards or mahjong, reading newspapers or books, keeping domestic animals or pets, and attending social activities. Our finding is in accordance with a previous study showing that older adults who engaged in a greater number of activities were less likely to die than were those who engaged in few activities [29]. Thus, encouraging older adults to participate in these activities can help reduce the risk of death.
- This study also provides evidence that contributes to explaining the mechanisms underlying the association between cognitive function and mortality and supports the view that leisure activities play an important role in this association. People with impaired cognitive function commonly have a combination of social isolation and depression [30,31], with which a loss of participation in social or physical leisure activities would occur after an early stage of cognitive deficit has developed owing to preclinical dementia. Discontinuing engagement in leisure activities may constitute an early sign of dementia incidence [32], and such potential dementia cases are more likely to experience cognitive decline eventually, resulting in higher rates of mortality. Thus, it’s a priority to reduce the risk of cognition-related mortality. It has been found that engaging in leisure activities could increase the resilience against the negative effects of cognitive impairment among those older adults and further reduce the mortality risk coming from cognitive impairment [27,33]. Additionally, previous studies have also put forward to 2 principles to guide engagement in leisure activities, that is, engaging in complex leisure activities and enabling people to engage in complex leisure activities at an early stage of cognitive impairment [34]. The effects of implementing these 2 principles for leisure activities have been confirmed in older people and patients with dementia [35]. Although the principles were developed on the basis of findings from Western countries, they are consistent with our results from older Chinses adults. Leisure activities are not a static property and they could be the target for intervention; improving leisure activities may contribute to protecting older people against cognitive decline and reducing the mortality risk that comes from cognitive impairment.
- We also evaluated the distinct causal effects of different types of leisure activities on the association between cognitive function and mortality. A previous study with 10,308 participants in the United Kingdom explicated that social leisure activities had a stronger and more consistent relationship with cognitive function and mortality than physical leisure activities [34]. The mechanisms may include support (received or provided), reduced depression, and positive emotions leading to the health-promoting physiological effects of decreased chronic sympatho-adrenal activation, improved immune function, and less chronic inflammation [36–38]. However, our results indicated that the PM for physical leisure activities was higher than that of social leisure activities. A plausible explanation for this finding is that physical leisure activities could increase the high-density lipoprotein level, reduce coronary artery calcium, and improve antioxidant defense systems [39]. It is also possibly explained by the different characteristics of older people between China and other countries. Combined with previous evidence, these results suggest that planned interventions for leisure activities, especially physical activities, at an early stage of mild cognitive impairment could promote health outcomes and optimally reduce the risk of mortality.
- Our results also suggest that leisure activities have a causal mediating effect on the association between cognitive function and mortality in different subgroups of age, educational attainment, lifestyle, and residence. We found that the PM of leisure activities in rural China was much higher than that in urban. Given the huge urban-rural differences in China, rural dwellers had fewer opportunities for social interactions, recreational facilities, and sports that are easily available to urban dwellers, resulting in poor cognitive performance and a higher risk of mortality [40], as well as a higher proportion mediated by leisure activities. Although these results reflect the relatively low availability of leisure resources and fewer choices for alternative activities in rural China, the findings from this study suggest that engagement in leisure activities might be more cost-effective for minimizing the risks of mortality associated with cognitive function in rural areas, in light of the relatively low degrees of leisure activities in those regions. Compared with the oldest old, the mediated magnitude for leisure activities was higher in younger-old adults in the present study. The results of our study have a similar pattern to previous work, according to which younger-old adults may develop cognitive impairment faster than the oldest-old [41]. Furthermore, it was observed that the association of cognitive impairment with mortality decreased with age in older Chinese cohorts [42]. Thus, whenever possible, early engagement in leisure activities for cognitively impaired younger-old adults may have a large impact on mortality in later life. Previously, education was found to play a moderating role in the relationship between cognitive performance and leisure activities in older adults [43]. Moreover, the relationship between cognitive function and leisure activities differed depending on the educational level; that is, the impacts of leisure activities on cognition were more profound for educated older people [22]. Our findings are consistent with those results that participating in leisure activities is more likely to reduce the risk of mortality for higher-educated older people. In addition, it is reasonable that the PM was higher in older adults with an unhealthy lifestyle than those with a healthy lifestyle, as older adults with unhealthy lifestyles are more likely to benefit from other healthy behaviors such as leisure activities [44].
- The results of this study have important implications for public health. Interventions at an early stage of cognitive impairment have been shown to be most effective, and even small effects may lead to significant public health benefits [45]. Many factors that contribute to the association between cognitive decline and mortality, such as advanced age and neurodegenerative diseases, are not modifiable. However, older people can readily modify their behaviors. By encouraging older people to participate in leisure activities, we can help to weaken the association between cognitive impairment and death. Based on longitudinal data, this study is the first of its kind to examine the mediating role of leisure activities on the association between cognitive function and mortality. A large sample size allowed us to adjust for a large number of covariates and conduct detailed analyses.
- Nonetheless, there are several limitations to this study. First, the MMSE is a brief measure of global cognitive function, which might not be sensitive enough. Second, we used the first interview date as a proxy for the date of diagnosis of cognitive impairment. Some patients may have been diagnosed a long time before our first interview, which may have affected their survival time, potentially biasing the results. Last, we did not exclude participants with cognitive impairment, which may increase the risk of reverse causality, as people in the very early stages of cognitive impairment may withdraw from social contact or other types of leisure activities. However, the use of longitudinal follow-up data and causal mediation models could counteract this risk to a certain extent.
- The present study showed a dose-response relationship between cognitive function and mortality. Leisure activities mediated this relationship. Early intervention for mild cognitive impairment, focusing mostly on physical leisure activities, could reduce the risk of mortality related to cognition.
DISCUSSION
SUPPLEMENTARY MATERIALS
ACKNOWLEDGEMENTS
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
The research results of this article are sponsored by Kunshan Municipal Government research funding.
-
AUTHOR CONTRIBUTIONS
Conceptualization: Chen X, Wu W, Yan LL, Yao Y. Data curation: Zhang X, Zhu W, Long T. Formal analysis: Chen X, Long T, Hu R. Funding acquisition: Yan LL. Methodology: Yan LL, Yao Y. Project administration: Yan LL, Yao Y. Visualization: Chen X, Jin X. Writing – original draft: Chen X, Wu W. Writing – review & editing: Chen X, Wu W, Jin X, Yan LL, Yao Y.
NOTES


| Characteristics |
Cognitive impairment1 |
||||||
|---|---|---|---|---|---|---|---|
| Not impaired | Mild | Moderate | Severe | Total | p-value | ||
| Total | 22,216 (52.6) | 8,855 (21.0) | 4,651 (11.0) | 6,524 (15.4) | 42,246 (100) | ||
| Age, median (25th, 75th) (yr) | 83 (75, 91) | 92 (85, 100) | 97 (91, 101) | 100 (94, 101) | 91 (80, 99) | <0.001 | |
| Sex | <0.001 | ||||||
| Male | 11,705 (52.7) | 2,948 (33.3) | 1,148 (24.7) | 1,465 (22.5) | 17,266 (40.9) | ||
| Female | 10,511 (47.3) | 5,907 (66.7) | 3,503 (75.3) | 5,059 (77.5) | 24,980 (59.1) | ||
| Educational attainment2 | <0.001 | ||||||
| No schooling | 11,338 (51.0) | 6,818 (77.0) | 3,974 (85.5) | 5,536 (84.8) | 27,666 (65.5) | ||
| Primary school | 6,263 (28.2) | 1,475 (16.7) | 513 (11.0) | 702 (10.8) | 8,953 (21.2) | ||
| Middle school or higher | 4,615 (20.8) | 562 (6.3) | 164 (3.5) | 286 (4.4) | 5,627 (13.3) | ||
| Main occupation before age 60 | <0.001 | ||||||
| Non-manual | 2,427 (10.9) | 254 (2.9) | 71 (1.5) | 143 (2.2) | 2,895 (6.9) | ||
| Manual | 19,789 (89.1) | 8,601 (97.1) | 4,580 (98.5) | 6,381 (97.8) | 39,351 (93.1) | ||
| Ethnicity | <0.001 | ||||||
| Han | 20,860 (93.9) | 8,318 (93.9) | 4,389 (94.4) | 6,217 (95.3) | 39,784 (94.2) | ||
| Others (minority) | 1,356 (6.1) | 537 (6.1) | 262 (5.6) | 307 (4.7) | 2,462 (5.8) | ||
| Residence | <0.001 | ||||||
| Urban | 10,041 (45.2) | 3,486 (39.4) | 1,689 (36.3) | 2,483 (38.1) | 17,699 (41.9) | ||
| Rural | 12,175 (54.8) | 5,369(60.6) | 2,962 (63.7) | 4,041(61.9) | 24,547 (58.1) | ||
| Marital status | <0.001 | ||||||
| Currently married and living with spouse | 8,555 (38.5) | 1,470 (16.6) | 373 (8.0) | 437 (6.7) | 10,835 (25.6) | ||
| Others3 | 13,661 (61.5) | 7,385 (83.4) | 4,278 (92.0) | 6,087 (93.3) | 31,411 (74.4) | ||
| Tobacco smoking status | <0.001 | ||||||
| Never | 13,353 (60.1) | 6,469 (73.1) | 3,652 (78.5) | 5,227 (80.1) | 28,701 (67.9) | ||
| Ever | 8,863 (39.9) | 2,386 (26.9) | 999 (21.5) | 1,297 (19.9) | 13,545 (32.1) | ||
| Alcohol drinking status | <0.001 | ||||||
| Never | 14,676 (66.1) | 6,361 (71.8) | 3,548 (76.3) | 4,978 (76.3) | 29,563 (70.0) | ||
| Ever | 7,540 (33.9) | 2,494 (28.2) | 1,103 (23.7) | 1,546 (23.7) | 12,683 (30.0) | ||
| Regular physical activity | <0.001 | ||||||
| Yes | 9,708 (43.7) | 2,754 (31.1) | 1,093 (23.5) | 1,448 (22.2) | 15,003 (35.5) | ||
| No | 12,508 (56.3) | 6,101 (68.9) | 3,558 (76.5) | 5,076 (77.8) | 27,243 (64.5) | ||
| Frequency of drinking tea | <0.001 | ||||||
| Every day or occasionally | 11,419 (51.4) | 3,781 (42.7) | 1,725 (37.1) | 1,990 (30.5) | 18,915 (44.8) | ||
| Rarely or never | 10,797 (48.6) | 5,074 (57.3) | 2,926 (62.9) | 4,534 (69.5) | 23,331 (55.2) | ||
| Lifestyle4 | <0.001 | ||||||
| Unhealthy | 10,930 (49.2) | 5,588 (63.1) | 3,195 (68.7) | 4,502 (69.0) | 24,215 (57.3) | ||
| Healthy | 11,286 (50.8) | 3,267 (36.9) | 1,456 (31.3) | 2,022 (31.0) | 18,031 (42.7) | ||
| Leisure activities, median (25th, 75th)5 | 13 (11, 15) | 11 (9, 13) | 10 (8, 11) | 9 (8, 10) | 12 (9, 14) | <0.001 | |
Values are presented as number (%).
MMSE, Mini-Mental State Examination.
1 Cognitive impairment was classified into 4 mutually exclusive groups: not impaired (25≤MMSE score≤30), mild (18≤MMSE score≤24), moderate (10≤MMSE score≤17), and severe (0≤MMSE score≤9) cognitive impairment.
2 Defined by years of schooling; None: school years=0; Primary school: school years=1-5; Middle school or higher: school years>5.
3 ‘Others’ include widowed, separated, divorced and never married.
4 The lifestyle score was calculated by the intake frequency of 10 food categories that have been demonstrated to be associated with cognitive function; A 3-point scale question was used to measure the current intake frequency of each food group: “always or almost every day,” “sometimes or occasionally,” or “rarely or never”; Those 3 terms received a score of 2, 1, or 0, respectively; The total score ranged from 0 to 20, and lifestyle was categorized as unhealthy or healthy using a cut-off score of 10.
5 The leisure activity score was calculated by 8 kinds of activities (housework, fieldwork, garden work, reading, pets, mahjong, television, social-activity) and we scored each activity 1 for “never,” 2 for “sometimes,” and 3 for “almost every day”; The score ranged from 6 to 24, with higher scores indicating more frequent leisure activities.
- 1. Andrews JS, Desai U, Kirson NY, Enloe CJ, Ristovska L, King S, et al. Functional limitations and health care resource utilization for individuals with cognitive impairment without dementia: findings from a United States population-based survey. Alzheimers Dement (Amst) 2016;6:65-74.ArticlePubMedPMCPDF
- 2. Weiler PG, Lubben JE, Chi I. Cognitive impairment and hospital use. Am J Public Health 1991;81:1153-1157.ArticlePubMedPMC
- 3. Tamosiunas A, Sapranaviciute-Zabazlajeva L, Luksiene D, Virviciute D, Bobak M. Cognitive function and mortality: results from kaunas HAPIEE Study 2006–2017. Int J Environ Res Public Health 2020;17:2397.ArticlePubMedPMC
- 4. Wang MC, Li TC, Li CI, Liu CS, Lin CH, Lin WY, et al. Cognitive function and its transitions in predicting all-cause mortality among urban community-dwelling older adults. BMC Psychiatry 2020;20:203.ArticlePubMedPMCPDF
- 5. Su Y, Dong J, Sun J, Zhang Y, Ma S, Li M, et al. Cognitive function assessed by Mini-mental state examination and risk of all-cause mortality: a community-based prospective cohort study. BMC Geriatr 2021;21:524.ArticlePubMedPMCPDF
- 6. Li Y, Jiang H, Jin X, Wang H, Ji JS, Yan LL. Cognitive impairment and all-cause mortality among Chinese adults aged 80 years or older. Brain Behav 2021;11:e2325.ArticlePubMedPMCPDF
- 7. Rajan KB, Aggarwal NT, Wilson RS, Everson-Rose SA, Evans DA. Association of cognitive functioning, incident stroke, and mortality in older adults. Stroke 2014;45:2563-2567.ArticlePubMedPMC
- 8. Dewey ME, Saz P. Dementia, cognitive impairment and mortality in persons aged 65 and over living in the community: a systematic review of the literature. Int J Geriatr Psychiatry 2001;16:751-761.ArticlePubMed
- 9. Zotcheva E, Selbæk G, Bjertness E, Ernstsen L, Strand BH. Leisure-time physical activity is associated with reduced risk of dementia-related mortality in adults with and without psychological distress: the cohort of Norway. Front Aging Neurosci 2018;10:151.ArticlePubMedPMC
- 10. Rijnhart JJ, Lamp SJ, Valente MJ, MacKinnon DP, Twisk JW, Heymans MW. Mediation analysis methods used in observational research: a scoping review and recommendations. BMC Med Res Methodol 2021;21:226.ArticlePubMedPMCPDF
- 11. Pearl J. Direct and indirect effects. Proceedings of the Seventeenth Conference on Uncertainty in Artificial Intelligence (UAI’01). San Francisco: Morgan Kaufmann Publishers Inc; 2001. 411-420.Article
- 12. Zeng Y, Feng Q, Gu D, Vaupel JW. Demographics, phenotypic health characteristics and genetic analysis of centenarians in China. Mech Ageing Dev 2017;165:86-97.ArticlePubMedPMC
- 13. An R, Liu GG. Cognitive impairment and mortality among the oldest-old Chinese. Int J Geriatr Psychiatry 2016;31:1345-1353.ArticlePubMed
- 14. Zeng Y, Feng Q, Hesketh T, Christensen K, Vaupel JW. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet 2017;389:1619-1629.ArticlePubMedPMC
- 15. Lv YB, Gao X, Yin ZX, Chen HS, Luo JS, Brasher MS, et al. Revisiting the association of blood pressure with mortality in oldest old people in China: community based, longitudinal prospective study. BMJ 2018;361:k2158.ArticlePubMedPMC
- 16. Nguyen HT, Black SA, Ray LA, Espino DV, Markides KS. Cognitive impairment and mortality in older mexican americans. J Am Geriatr Soc 2003;51:178-183.ArticlePubMed
- 17. Mungas D. In-office mental status testing: a practical guide. Geriatrics 1991;46:54-58. 63. 66.
- 18. Zhang Z, Gu D, Hayward MD. Childhood nutritional deprivation and cognitive impairment among older Chinese people. Soc Sci Med 2010;71:941-949.ArticlePubMedPMC
- 19. Lv X, Li W, Ma Y, Chen H, Zeng Y, Yu X, et al. Cognitive decline and mortality among community-dwelling Chinese older people. BMC Med 2019;17:63.ArticlePubMedPMCPDF
- 20. Zhang Y, Fu S, Ding D, Lutz MW, Zeng Y, Yao Y. Leisure activities, APOE ɛ4, and cognitive decline: a longitudinal cohort study. Front Aging Neurosci 2021;13:736201.ArticlePubMedPMC
- 21. Teh JK, Tey NP. Effects of selected leisure activities on preventing loneliness among older Chinese. SSM Popul Health 2019;9:100479.ArticlePubMedPMC
- 22. Zhu X, Qiu C, Zeng Y, Li J. Leisure activities, education, and cognitive impairment in Chinese older adults: a population-based longitudinal study. Int Psychogeriatr 2017;29:727-739.ArticlePubMedPMC
- 23. Robins JM, Greenland S. Identifiability and exchangeability for direct and indirect effects. Epidemiology 1992;3:143-155.ArticlePubMed
- 24. VanderWeele TJ. A three-way decomposition of a total effect into direct, indirect, and interactive effects. Epidemiology 2013;24:224-232.ArticlePubMedPMC
- 25. Yoshida K, Mathur M, Glynn RJ. Conducting regression-based causal mediation analysis using the R package “regmedint”. OSF Preprints. [Preprint]. 2020 [cited 2020 Nov 9]. Available from: https://doi.org/10.31219/osf.io/6c79f .Article
- 26. Eisele M, Zimmermann T, Köhler M, Wiese B, Heser K, Tebarth F, et al. Influence of social support on cognitive change and mortality in old age: results from the prospective multicentre cohort study AgeCoDe. BMC Geriatr 2012;12:9.ArticlePubMedPMCPDF
- 27. Yu H. Universal health insurance coverage for 1.3 billion people: what accounts for China’s success? Health Policy 2015;119:1145-1152.ArticlePubMedPMC
- 28. Hai S, Cao L, Yang X, Wang H, Liu P, Hao Q, et al. Association between nutrition status and cognitive impairment among Chinese nonagenarians and centenarians. Int J Gerontol 2017;11:215-219.Article
- 29. Obisesan TO, Gillum RF. Cognitive function, social integration and mortality in a U.S. national cohort study of older adults. BMC Geriatr 2009;9:33.ArticlePubMedPMCPDF
- 30. Wilson RS, Mendes De Leon CF, Bennett DA, Bienias JL, Evans DA. Depressive symptoms and cognitive decline in a community population of older persons. J Neurol Neurosurg Psychiatry 2004;75:126-129.PubMedPMC
- 31. Kim OS, Yang SJ, Kim JH, Kim NY, Jeon HO. Leisure activities, cognitive function and depression in female elderly. Korean J Adult Nurs 2007;19:436-446 (Korean)..
- 32. Fratiglioni L, Paillard-Borg S, Winblad B. An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol 2004;3:343-353.ArticlePubMed
- 33. Katja P, Timo T, Taina R, Tiina-Mari L. Do mobility, cognitive functioning, and depressive symptoms mediate the association between social activity and mortality risk among older men and women? Eur J Ageing 2013;11:121-130.ArticlePubMedPMCPDF
- 34. Singh-Manoux A, Richards M, Marmot M. Leisure activities and cognitive function in middle age: evidence from the Whitehall II study. J Epidemiol Community Health 2003;57:907-913.ArticlePubMedPMC
- 35. Koh K, Ray R, Lee J, Nair A, Ho T, Ang PC. Dementia in elderly patients: can the 3R mental stimulation programme improve mental status? Age Ageing 1994;23:195-199.ArticlePubMed
- 36. Krause N. Church-based social support and mortality. J Gerontol B Psychol Sci Soc Sci 2006;61:S140-S146.ArticlePubMed
- 37. Lutgendorf SK, Russell D, Ullrich P, Harris TB, Wallace R. Religious participation, interleukin-6, and mortality in older adults. Health Psychol 2004;23:465-475.ArticlePubMed
- 38. Ford ES, Loucks EB, Berkman LF. Social integration and concentrations of C-reactive protein among US adults. Ann Epidemiol 2006;16:78-84.ArticlePubMed
- 39. Friedenreich CM, Orenstein MR. Physical activity and cancer prevention: etiologic evidence and biological mechanisms. J Nutr 2002;132(11 Suppl):3456S-3464S.ArticlePubMed
- 40. Duan J, Lv YB, Gao X, Zhou JH, Kraus VB, Zeng Y, et al. Association of cognitive impairment and elderly mortality: differences between two cohorts ascertained 6-years apart in China. BMC Geriatr 2020;20:29.ArticlePubMedPMCPDF
- 41. Bassuk SS, Wypij D, Berkman LF. Cognitive impairment and mortality in the community-dwelling elderly. Am J Epidemiol 2000;151:676-688.ArticlePubMed
- 42. Park S, Choi B, Choi C, Kang JM, Lee JY. Relationship between education, leisure activities, and cognitive functions in older adults. Aging Ment Health 2019;23:1651-1660.ArticlePubMed
- 43. Xu H, Vorderstrasse AA, Dupre ME, McConnell ES, Østbye T, Wu B. Gender differences in the association between migration and cognitive function among older adults in China and India. Arch Gerontol Geriatr 2019;81:31-38.ArticlePubMed
- 44. Bosma H, van Boxtel MP, Ponds RW, Jelicic M, Houx P, Metsemakers J, et al. Engaged lifestyle and cognitive function in middle and old-aged, non-demented persons: a reciprocal association? Z Gerontol Geriatr 2002;35:575-581.ArticlePubMedPDF
- 45. Leung GT, Fung AW, Tam CW, Lui VW, Chiu HF, Chan WM, et al. Examining the association between participation in late-life leisure activities and cognitive function in community-dwelling elderly Chinese in Hong Kong. Int Psychogeriatr 2010;22:2-13.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
- Cognitive performance and all-cause mortality in community dwellers of Amerindian ancestry living in rural Ecuador: A population-based, longitudinal prospective study
Oscar H. Del Brutto, Denisse A. Rumbea, Aldo F. Costa, Maitri Patel, Mark J. Sedler, Robertino M. Mera
Clinical Neurology and Neurosurgery.2024; 236: 108053. CrossRef - Change in Healthy Lifestyle and Subsequent Risk of Cognitive Impairment Among Chinese Older Adults: A National Community-Based Cohort Study
Chengxiang Hu, Kexin Jiang, Xiaoyue Sun, Yue He, Runhong Li, Yana Chen, Yuan Zhang, Yuchun Tao, Lina Jin, Lewis A Lipsitz
The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences.2024;[Epub] CrossRef - Healthy lifestyle in late-life, longevity genes, and life expectancy among older adults: a 20-year, population-based, prospective cohort study
Jun Wang, Chen Chen, Jinhui Zhou, Lihong Ye, Yang Li, Lanjing Xu, Zinan Xu, Xinwei Li, Yuan Wei, Junxin Liu, Yuebin Lv, Xiaoming Shi
The Lancet Healthy Longevity.2023; 4(10): e535. CrossRef - Associations of Unhealthy Lifestyle and Nonalcoholic Fatty Liver Disease With Cardiovascular Healthy Outcomes
Wentao Wu, Wen Ma, Shiqi Yuan, Aozi Feng, Li Li, Haoxiao Zheng, Shuna Li, Ningxia He, Yuli Huang, Jun Lyu
Journal of the American Heart Association.2023;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite



