Articles
- Page Path
- HOME > Epidemiol Health > Volume 44; 2022 > Article
-
Data Profile
The National Hospice and Palliative Care registry in Korea -
Kyuwoong Kim
 , Bohyun Park, Bonju Gu, Eun Jeong Nam, Sue Hyun Kye, Jin Young Choi
, Bohyun Park, Bonju Gu, Eun Jeong Nam, Sue Hyun Kye, Jin Young Choi -
Epidemiol Health 2022;44:e2022079.
DOI: https://doi.org/10.4178/epih.e2022079
Published online: September 21, 2022
National Hospice Center, National Cancer Control Institute, National Cancer Center, Goyang, Korea
- Correspondence: Jin Young Choi National Hospice Center, National Cancer Control Institute, National Cancer Center, 323 Ilsan-ro, Ilsandong-gu, Goyang 10408, Korea E-mail: ilotopie@ncc.re.kr
© 2022 Korea Disease Control and Prevention Agency.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- The National Hospice and Palliative Care (NHPC) registry is a nationwide database in Korea that systematically collects information on terminally ill cancer patients receiving inpatient hospice care. From 2018 to 2020, a total of 47,911 patients were enrolled in the NHPC registry from hospitals providing inpatient hospice care. The NHPC database mainly contains the socio-demographic and clinical information of the registered patients. Among these patients, approximately 75% were 60 years or older, and the ratio of males to females was 1:1.41. Lung, liver, colorectal, pancreatic, and gastric cancer made up nearly 90% of the cancer sites among the registered patients. Upon their initial admission to the hospice ward, around 80% of the patients were aware of their terminal illness. About half of the patients had mild pain at the time of the initial admission to the hospice ward, and the duration of hospice care was 14 days (interquartile range, 6-30) in 2019 and 2020. The NHPC registry aims to provide national statistics on inpatient hospice care to assist health policy-making.
- Cancer is consistently among the major leading causes of death in Korea and elsewhere in the world despite some variations across countries by income level [1-3]. Compared to the previous year, cancer mortality increased by 1.2% in Korea in 2019, and cancer remained the leading cause of death, followed by cerebrovascular accidents [4,5]. However, there is a paucity of data on the most up-to-date national statistics on hospice and palliative care (HPC) in the previous literature. Among those who died from cancer, approximately 15% were reported to have been newly admitted to hospitals to receive inpatient hospice care at the end-of-life (EoL) in Korea in 2015 [6]. A previous study [7] describing terminally ill cancer patients receiving inpatient hospice care registered in the Korean Terminal Cancer Patient Information System (KTCPIS) was conducted in 2009. In addition to the outdated information describing the status of HPC, the KTCPIS is no longer in use for registering terminally ill cancer patients. Furthermore, the Act on Decisions on Life-sustaining Treatment for Patients in Hospice and Palliative Care or at the End of Life was enacted and enforced in 2016 and 2017, respectively [8]. In accordance with the Act, the National Hospice Center (NHC) was designated by the Ministry of Health and Welfare to collect, analyze, and provide statistics on the status of HPC in Korea [9].
- This study aimed to describe the most up-to-date data collection procedure and components of the database derived from the National Hospice and Palliative Care (NHPC) registry, which is used to provide nationwide statistics on HPC in Korea.
INTRODUCTION
- The National Hospice and Palliative Care database
- The NHPC registry was constructed to collect information and provide national statistics on patients at the EoL receiving HPC in Korea. The NHC at the National Cancer Center has been managing the NHPC registration system and database since 2017 and has published annual reports of HPC statistics. The NHPC registration system undergoes information system management and improvement on a regular basis to integrate the data collected from nearly 100 hospitals designated by the Ministry of Health and Welfare to provide HPC to terminally ill cancer patients. In accordance with Article 21 of the Act on Decisions on Life-sustaining Treatment for Patients in Hospice and Palliative Care or at the End of Life, the NHC is able to construct a nationwide database related to HPC among patients at the EoL.
DATA RESOURCE
- The National Hospice and Palliative Care Study
- The currently operating NHPC registration system collects data on the terminally ill cancer patients using a common case report form (CRF) due to large variations in the data structure of the electronic medical record (EMR) system in each hospital that provides HPC. Prior to the implementation of the NHPC system, the CRF was both internally and externally reviewed by experts. To obtain and abstract data on socio-demographic factors, the initial assessment (i.e., clinical evaluation) of the patients, and death records, each hospital is required to review the EMR and submit appropriate data to the NHPC registration system on a regular basis. The cancer site of each patient was classified according to the Korean Standard Classification of Diseases-6 (KCD-6), which is comparable to the International Classification of Diseases, 10th revision (ICD-10). As most terminally ill cancer patients need extensive care, information on the primary caregiver, such as the legal relationship and whether the patient was living together with the caregiver prior to hospitalization, was collected. The key variables of the NHPC database are presented in Table 1.
- Among the hospitals that specialize in providing inpatient hospice care, terminally ill cancer patients who were newly registered and began to receive HPC were enrolled in the NHPC registration system between 2018 and 2020. The assessment of terminal illness was determined by the physician in charge as well as the specialist in the relevant field according to clinical symptoms, the presence of other diseases or disorders, the degree of improvement due to drug administration or procedures, the progress of previous medical treatment, and availability of other treatment options for the patient. A total of 15,859 patients were enrolled in 2018, and 16,798 were enrolled in 2019, which was an increase of 5.9% compared to the year before. In 2020, the number of patients enrolled in the system was similar to that of 2018 (n= 15,254) (Table 2). No probability sampling method was necessary in the process of selecting enrollees because the NHPC registration system included virtually all terminally ill cancer patients receiving HPC in Korea.
- Data collection
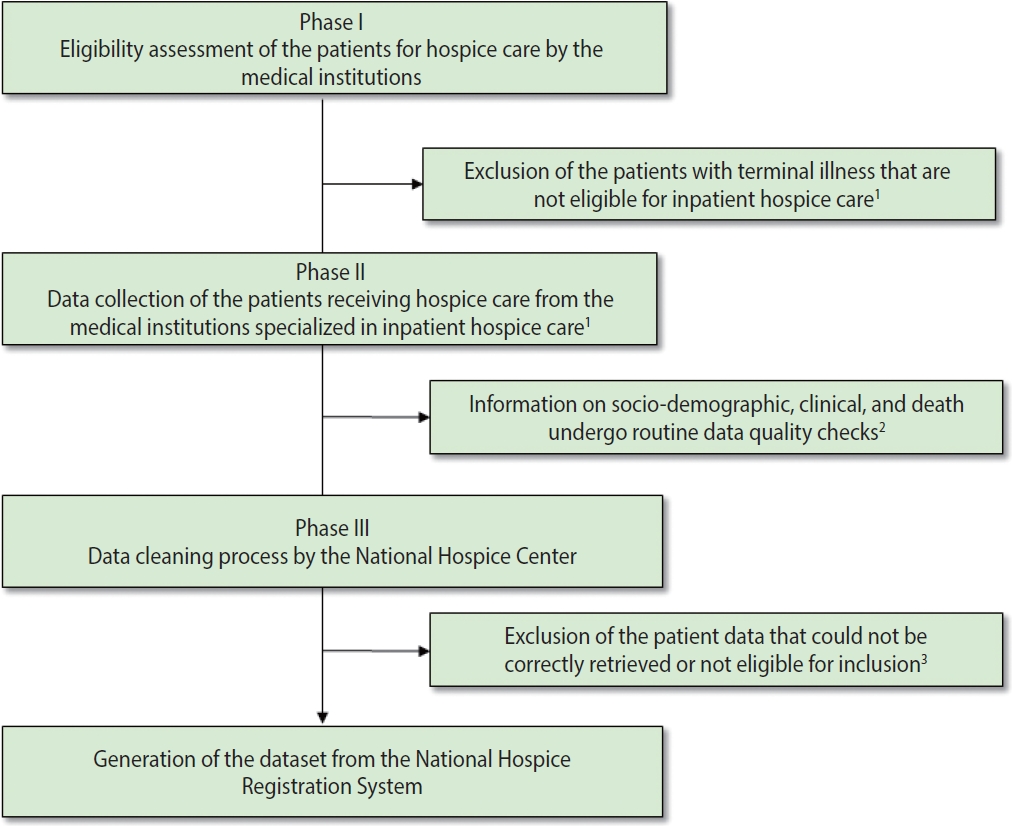
- Currently, only terminally ill cancer patients are eligible for inpatient hospice care in Korea under the Article 2 of the Act on Decisions on Life-sustaining Treatment for Patients in Hospice and Palliative Care or at the End of Life. Accordingly, data on cancer patients who have limited life expectancy (i.e., without any possibility of recovery and who are expected to die within a few months) confirmed by medical doctors are collected through the NHPC registry. Prior to generating the final dataset used for producing national statistics on HPC, the collected data in the NHPC undergo data quality checks from the initial eligibility assessment to data cleaning (Figure 1). Employees of the NHC who are in charge of data collection routinely identify data in the NHPC registration system that might have been incorrectly entered based on the EMR from each hospital. From 2018 to 2020, there were around 100 hospitals from which nationwide data on HPC were collected (98 hospitals with a total of 1,542 hospice beds in 2018, 100 hospitals with a total of 1,577 beds in 2019, and 97 hospitals with a total of 1,546 beds in 2020, respectively). If a hospital providing inpatient hospice care was revoked of its designation status (i.e., as a specialized medical institution providing inpatient hospice care) by the Ministry of Health and Welfare or temporarily closed (i.e., due to the coronavirus disease 2019 pandemic or other reasons) data from that hospital were not included in the NHPC registry. In addition, data with suspicious values that could not be correctly retrieved by contacting the person in charge at each hospital were also excluded as of the last calendar date in each year. Thus, the NHPC registry only contains quality-assured nationwide data on inpatient hospice care.
- Ethics statement
- The study protocol for the NHPC registry was approved by the Institutional Review Board at the National Cancer Center, Goyang, Korea (IRB No. NCCNCS09234). Written informed consent was obtained from each patient or his or her legal guardian upon registration. Administrative permission to access the NHPC registry was only granted to authorized personnel who were approved by the appropriate ethics committee of each hospital. The study protocol adhered to the legal regulations of Korea and was also in compliance with the Declaration of Helsinki.
MEASURES
Structure of the dataset
Selection of the enrollees
- Socio-demographic characteristics of the enrollees
- From January 1, 2018 to December 31, 2020, a total of 47,911 terminally ill cancer patients were enrolled at 97 hospitals providing inpatient hospice care (as of 2020) in Korea. The socio-demographic characteristics of the newly registered patients receiving inpatient hospice care from 2018 to 2020 are shown in Table 3. Most patients (≥ 75%) were aged 60 years or more, and approximately 58% of the patients were male. More than two-thirds of the patients resided in the capital area or metropolitan area, and nearly 90% of them were covered by the National Health Insurance Service (i.e., employee-insured and self-employed insured), whereas around 9% of them were recipients of the Medical Aid program. Nearly 65% of the patients were married, and approximately 30% of them were either bereaved of their spouses or divorced at the time of enrollment. Fewer than 5% of the patients were single (i.e., not legally married) or separated (i.e., living separately regardless of the marital status). Among the patients who were reported to be religious, Protestantism was the most common religion (24.6 to 26.7%) followed by Buddhism (17.0 to 17.9%) and Catholicism (12.1 to 13.5%). Around 40% of the patients reported that they had no religious background at all. Family caregiving was the most common practice among the patients (92.2 to 95.5%). The distribution of patients’ socio-demographic characteristics remained consistent throughout the years.
- Clinical characteristics of the enrollees
- Table 4 demonstrates the clinical characteristics of the patients enrolled in inpatient hospice care between 2018 and 2020. Among these patients, nearly 90% of the cancer sites were non-sex-specific. Lung cancer (ICD-10: C34) was the most common type of cancer among the terminally ill cancer patients (15.7-18.7%), followed by liver cancer (ICD-10: C22; 10.6-11.7%) and colorectal cancer (ICD-10: C18-C20; 10.3-11.5%), pancreatic cancer (ICD-10: C25; 9.4-11.0%), and gastric cancer (ICD-10: C16; 8.8-10.1%). Nearly 80% of the patients were aware of their medical condition (i.e., of the fact that they had terminal cancer that could not be cured or treated). This proportion steadily increased from 2018 to 2020 (81.6% in 2018, 82.9% in 2019, and 85.5% in 2020). The level of consciousness among the patients at the time of initial assessment was fairly consistent throughout the years. Most (≥ 70%) of the patients were alert when they were first admitted to the hospice ward, and nearly a quarter of them were drowsy (18.3 to 20.6%) or stuporous (5.7 to 6.5%). Fewer than 1% of them were in a coma upon admission (0.7% in 2019 and 0.8% in 2018 and 2020, respectively). About half of the patients had mild pain at the time of initial registration in the inpatient hospice ward on a scale of 0 to 10 (i.e., 0: none, 1-3: mild, 4-6: moderate, and 7-10: severe). The median duration of inpatient hospice care (i.e., from the initial admission to discharge) was 15 days (interquartile range [IQR], 6-31) in 2018 and 14 days (IQR, 6-30) in 2019 and 2020, respectively.
- National hospice and palliative care statistics
- Currently, the NHPC registry is mostly used for producing national statistics on HPC in Korea. Notably, the hospice utilization rate is calculated by the number of newly registered patients receiving HPC divided by the number of cancer deaths. On an annual basis, the number of cancer deaths is reported in the Causes of Death Registry by Statistics Korea. The hospice utilization rate among cancer patients was 22.9% (2018), 24.3% (2019), and 23.0% (2020), respectively. The number of hospital beds assigned for HPC per 1,000,000 people is also computed for each administrative district using the population size reported by Statistics Korea (Population and Housing Census). As of 2020, the number of hospital beds assigned for HPC was 30 per 1,000,000 people in Korea. The province with the highest number was Jeonbuk (54 hospital beds for HPC per 1,000,000 people) and the lowest was Jeju (13 hospital beds for HPC per 1,000,000 people). In the capital city area (Seoul, Gyeonggi, and Incheon), the number of hospital beds for HPC per 1,000,000 people was around 27 to 30 (Figure 2).
DATA RESOURCE USE
- The most notable strength of the NHPC registry in Korea is its representativeness, which derives from collecting nationwide data on terminally ill cancer patients receiving HPC. The NHC has been providing reliable statistics on the current status of HPC in Korea. In North America and Europe, nationwide databases on HPC are rarely reported or limited to certain population groups [10]. For instance, the Center for Medicare and Medicaid Services (CMS) of the United States provides a hospice care data archive and releases relevant statistics [11]. The CMS database on hospice comprises elderly (65 years or older) Medicare beneficiaries [12]. Thus, the reports on Medicare patients enrolled in hospice programs are limited to a certain age group and insurance type in the United States [13]. Additional strengths include the high validity of the cancer diagnosis codes and the rigorous quality check procedures for constructing the database and the ability to compute national statistics on HPC combined with other sources of information provided by Statistics Korea without any data linkage (i.e., the hospice utilization rate and the number of hospital beds assigned for HPC can be calculated without linkage to the Death Registry or the Population and Housing Census).
- Some limitations of the NHPC database should also be noted. The NHPC registry only enrolls terminally ill cancer patients who received inpatient hospice care. Thus, information on a control group (e.g., a similar group of terminally ill cancer patients admitted to the intensive care unit in the same hospital or elsewhere) is unknown, and this resource cannot be used to compare sociodemographic and clinical characteristics or EoL outcomes to those who received HPC [14]. Additionally, marital status and religion are self-reported (either by a patient or his or her legal guardian) without further validation. However, such information is usually only self-reported in other well-established population-based registries, such as the Community Health Survey and the Nurses’ Health Study [15,16].
STRENGTHS AND WEAKNESSES
- The National Hospice Center developed a website for releasing national HPC statistics in Korea (https://www.hospice.go.kr). Currently, a part of the National Hospice and Palliative Care database is available from the Public Data Portal (https://www.data.go.kr) managed by the Ministry of the Interior and Safety. The National Hospice Center regularly updates this information after a careful and comprehensive review.
DATA ACCESSIBILITY
- To produce national statistics of terminally ill cancer patients receiving inpatient hospice care, the NHPC registry was implemented. This registry and collects nationwide data in Korea on a regular basis that undergo extensive quality checks. The NHPC database consists of information on patients’ socio-demographic and clinical characteristics. The NHPC database is often used to address the current status of inpatient hospice care and serves as an important part of the real-world evidence associated with terminally ill cancer patients for policy-makers and other stakeholders.
CONCLUSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This study was supported by the National Cancer Center in Korea (grant No. NCC-2211830-1).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Kim K, Choi JY. Data curation: Gu B. Formal analysis: Kim K, Gu B. Funding acquisition: Choi JY. Methodology: Kim K, Park B, Gu B. Project administration: Kim K, Choi JY. Writing – original draft: Kim K. Writing-review & editing: Kim K, Park B, Gu B, Nam EJ, Kye S, Choi JY.
NOTES
ACKNOWLEDGEMENTS

| Dataset | Variables |
|---|---|
| Patient socio-demographics | Basic information (name, sex, and resident registration number, location of residence), insurance type, marital status, religion, information on the primary caregiver1 |
| Initial assessment of the patient | Information on terminal illness2, diagnosis date, KCD-6 codes, patient‘s awareness, clinical evidence for the diagnosis, level of consciousness, date of hospitalization, patient status upon hospital admission, pain scale3, date of discharge, reason for discharge |
| Hospice care duration | Duration of inpatient hospice care |
KCD-6, Korean Standard Classification of Diseases-6.
1 Legally defined relationship (between the patient and caregiver) and whether the patient is living together with the primary caregiver or not.
2 Defined as an end-stage illness that is legally eligible for hospice care (cancer for inpatient hospice care).
3 Assessed at the time of the initial admission to the hospice ward.
| Category | 2018 | 2019 | 2020 |
|---|---|---|---|
| Total no. of patients1 | 15,859 | 16,798 | 15,254 |
| Medical institutions2 | - | - | - |
| Total no. | 98 | 100 | 97 |
| No. of beds3 | 1,542 | 1,577 | 1,546 |
| Variable | 2018 | 2019 | 2020 |
|---|---|---|---|
| No. of patients | 15,859 | 16,798 | 15,254 |
| Age (yr) | |||
| <39 | 277 (1.7) | 256 (1.5) | 233 (1.5) |
| 40-49 | 867 (5.5) | 878 (5.2) | 744 (4.9) |
| 50-59 | 2,319 (14.6) | 2,484 (14.8) | 2,095 (13.7) |
| 60-69 | 3,710 (23.4) | 3,941 (23.5) | 3,775 (24.7) |
| ≥70 | 8,686 (54.8) | 9,239 (55.0) | 8,407 (55.1) |
| Sex | |||
| Male | 9,250 (58.3) | 9,766 (58.2) | 8,929 (58.5) |
| Female | 6,609 (41.7) | 7,032 (41.8) | 6,325 (41.5) |
| Location of residence | |||
| Capital area | 7,506 (47.3) | 7,773 (46.2) | 6,865 (45.0) |
| Metropolitan | 3,384 (21.3) | 3,655 (21.8) | 3,715 (24.4) |
| Rural (city/town) | 4,969 (31.4) | 5,370 (32.0) | 4,674 (30.6) |
| Insurance type | |||
| NHIS1 | 14,274 (90.0) | 15,137 (90.1) | 13,766 (90.2) |
| Medical Aid | 1,383 (8.7) | 1,485 (8.8) | 1,354 (8.9) |
| Other | 202 (1.3) | 176 (1.0) | 134 (0.9) |
| Marital status | |||
| Married | 10,391 (65.5) | 10,834 (64.5) | 9,909 (65.0) |
| Bereaved | 3,454 (21.8) | 3,666 (21.8) | 3,225 (21.1) |
| Divorced | 1,175 (7.4) | 1,343 (8.0) | 1,307 (8.6) |
| Single | 694 (4.4) | 815 (4.9) | 702 (4.6) |
| Separation | 145 (0.9) | 140 (0.8) | 111 (0.7) |
| Religion | |||
| Protestantism | 4,178 (26.3) | 4,487 (26.7) | 3,746 (24.6) |
| Buddhism | 2,835 (17.9) | 2,851 (17.0) | 2,713 (17.8) |
| Catholicism | 2,047 (12.9) | 2,264 (13.5) | 1,842 (12.1) |
| Others | 234 (1.5) | 273 (1.6) | 245 (1.6) |
| None | 6,565 (41.4) | 6,923 (41.2) | 6,708 (44.0) |
| Primary caregiver | |||
| Family | 15,153 (95.5) | 15,949 (94.9) | 14,066 (92.2) |
| Others | 706 (4.5) | 849 (5.1) | 1,188 (7.8) |
| Variable | 2018 | 2019 | 2020 |
|---|---|---|---|
| No. of patients | 15,859 | 16,798 | 15,254 |
| Cancer types | |||
| Lung | 2,482 (15.7) | 2,943 (17.5) | 2,849 (18.7) |
| Liver | 1,679 (10.6) | 1,961 (11.7) | 1,760 (11.5) |
| Colorectal | 1,627 (10.3) | 1,928 (11.5) | 1,713 (11.2) |
| Pancreas | 1,485 (9.4) | 1,814 (10.8) | 1,674 (11.0) |
| Gastric | 1,394 (8.8) | 1,701 (10.1) | 1,508 (9.9) |
| Others1 | 7,192 (45.3) | 6,451 (38.4) | 5,750 (37.7) |
| Awareness of terminal illness (patients) | 12,940 (81.6) | 13,930 (82.9) | 13,045 (85.5) |
| Level of consciousness | |||
| Alert | 11,814 (74.5) | 12,412 (73.9) | 11,002 (72.1) |
| Drowsy | 2,910 (18.3) | 3,314 (19.7) | 3,147 (20.6) |
| Stuporous | 1,009 (6.4) | 960 (5.7) | 985 (6.5) |
| Comatose | 126 (0.8) | 112 (0.7) | 120 (0.8) |
| Pain assessment at the time of initial registration2 | |||
| 0 (none) | 1,075 (11.2) | 914 (9.4) | 697 (8.1) |
| 1-3 (mild) | 4,910 (51.0) | 5,090 (52.5) | 4,570 (53.2) |
| 4-6 (moderate) | 2,638 (27.4) | 2,790 (28.8) | 2,442 (28.4) |
| 7-10 (severe) | 1,001 (10.4) | 910 (9.4) | 875 (10.2) |
| Duration of hospice care, days (median, IQR) | 15 (6-31) | 14 (6-30) | 14 (6-30) |
- 1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209-249.ArticlePubMedPDF
- 2. Dagenais GR, Leong DP, Rangarajan S, Lanas F, Lopez-Jaramillo P, Gupta R, et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study. Lancet 2020;395:785-794.ArticlePubMed
- 3. Sidney S, Go AS, Rana JS. Transition from heart disease to cancer as the leading cause of death in the United States. Ann Intern Med 2019;171:225.Article
- 4. Kang MJ, Won YJ, Lee JJ, Jung KW, Kim HJ, Kong HJ, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2019. Cancer Res Treat 2022;54:330-344.ArticlePubMedPMCPDF
- 5. Vital Statistics Division; Statistics Korea, Shin HY, Kim J, Lee S, Park MS, Park S, et al. Cause-of-death statistics in 2018 in the Republic of Korea. J Korean Med Assoc 2020;63:286-297.ArticlePDF
- 6. Kim CG. Hospice & palliative care policy in Korea. Korean J Hosp Palliat Care 2017;20:8-17 (Korean).ArticlePDF
- 7. Shin DW, Choi JY, Nam BH, Seo WS, Kim HY, Hwang EJ, et al. The current status of utilization of palliative care units in Korea: 6 month results of 2009 Korean terminal cancer patient information system. Korean J Hosp Palliat Care 2010;13:181-189 (Korean).Article
- 8. Kim SH. Act on decisions on life-sustaining treatment. Korean J Fam Pract 2021;11:323-323 (Korean).Article
- 9. Kim CG. The history of hospice and palliative care in Korea. Korean J Hosp Palliat Care 2019;22:1-7 (Korean).Article
- 10. Fine PG. Hospice underutilization in the U.S.: the misalignment of regulatory policy and clinical reality. J Pain Symptom Manage 2018;56:808-815.ArticlePubMed
- 11. Berwick DM, Gilfillan R. Reinventing the center for Medicare and Medicaid innovation. JAMA 2021;325:1247-1248.ArticlePubMed
- 12. Odejide OO. A policy prescription for hospice care. JAMA 2016;315:257-258.ArticlePubMed
- 13. Hughes MC, Vernon E. Closing the gap in hospice utilization for the minority Medicare population. Gerontol Geriatr Med 2019;5:2333721419855667.ArticlePubMedPMCPDF
- 14. Pyenson B, Connor S, Fitch K, Kinzbrunner B. Medicare cost in matched hospice and non-hospice cohorts. J Pain Symptom Manage 2004;28:200-210.ArticlePubMed
- 15. Kim H, Lee K, Chang S, Kang G, Tak Y, Lee M, et al. Factors affecting the validity of self-reported data on health services from the community health survey in Korea. Yonsei Med J 2013;54:1040-1048.ArticlePubMedPMC
- 16. Zhang Z, Laden F, Forman JP, Hart JE. Long-term exposure to particulate matter and self-reported hypertension: a prospective analysis in the Nurses’ Health Study. Environ Health Perspect 2016;124:1414-1420.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- For the Universal Right to Access Quality End-of-Life Care in Korea: Broadening Our Perspective After the 2018 Life-Sustaining Treatment Decisions Act
Hye Yoon Park, Min Sun Kim, Shin Hye Yoo, Jung Lee, In Gyu Song, So Yeon Jeon, Eun Kyung Choi
Journal of Korean Medical Science.2024;[Epub] CrossRef - Differences in end-of-life care patterns between types of hospice used for cancer patients: a retrospective cohort study
Il Yun, Eun-Cheol Park, Chung Mo Nam, Jaeyong Shin, Suk-Yong Jang, Sung-In Jang
BMC Palliative Care.2024;[Epub] CrossRef - Inpatient Hospice Care in Korea during the COVID-19 Pandemic: A Preliminary Study
Youn Seon Choi, Sun Wook Hwang, In Cheol Hwang
Journal of Hospice and Palliative Care.2024; 27(2): 82. CrossRef - Decreased aggressive care at the end of life among advanced cancer patients in the Republic of Korea: a nationwide study from 2012 to 2018
Sara Kwon, Kyuwoong Kim, Bohyun Park, So-Jung Park, Hyun Jung Jho, Jin Young Choi
BMC Palliative Care.2024;[Epub] CrossRef - Advance Care Planning in South Korea
Yu Jung Kim, Sun-Hyun Kim
Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen.2023; 180: 68. CrossRef - Changes in the Place of Death of Patients With Cancer After the Introduction of Insurance-Covered, Home-Based Hospice Care in Korea
Il Yun, Sung-In Jang, Eun-Cheol Park, Suk-Yong Jang
JAMA Network Open.2023; 6(11): e2341422. CrossRef - Application of Acceptance and Commitment Therapy (ACT) in Hospice and Palliative Care Settings
So-Young Park
The Journal of Hospice and Palliative Care.2023; 26(3): 140. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite