
Articles
- Page Path
- HOME > Epidemiol Health > Volume 44; 2022 > Article
-
COVID-19
Brief Communication
Trends in gastrointestinal infections before and during non-pharmaceutical interventions in Korea in comparison with the United States -
Soyeoun Kim1
 , Jinhyun Kim2, Bo Youl Choi3, Boyoung Park3
, Jinhyun Kim2, Bo Youl Choi3, Boyoung Park3 -
Epidemiol Health 2022;44:e2022011.
DOI: https://doi.org/10.4178/epih.e2022011
Published online: January 3, 2022
1Department of Health Sciences, Hanyang University College of Medicine, Seoul, Korea
2Economics & Business Economics, University of Amsterdam, Amsterdam, The Netherlands
3Department of Preventive Medicine, Hanyang University College of Medicine, Seoul, Korea
- Correspondence: Boyoung Park Department of Preventive Medicine, Hanyang University College of Medicine, 222 Wangsimni-ro, Seongdong-gu, Seoul 04763, Korea E-mail: hayejine@hanmail.net
©2022, Korean Society of Epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
OBJECTIVES
- This study examined how trends in the weekly frequencies of gastrointestinal infectious diseases changed before and during the coronavirus disease 2019 (COVID-19) pandemic in Korea, and compared them with the trends in the United States.
-
METHODS
- We compared the weekly frequencies of gastrointestinal infectious diseases (16 bacterial and 6 viral diseases) in Korea during weeks 5-52 before and after COVID-19. In addition, the weekly frequencies of 5 gastrointestinal infectious diseases in the United States (data from the Centers for Disease Control and Prevention) that overlapped with those in Korea were compared.
-
RESULTS
- The mean weekly number of total cases of gastrointestinal infectious diseases in Korea showed a significant decrease (from 522 before COVID-19 to 245 after COVID-19, p<0.01). Only bacterial gastrointestinal infectious diseases caused by Campylobacter increased significantly; other bacterial gastrointestinal infectious diseases showed either a decrease or no change. The incidence of all other viral diseases decreased. In the United States, the weekly numbers of Salmonella, Campylobacter, typhoid, shigellosis, and hepatitis A virus cases sharply decreased after the COVID-19 outbreak. The weekly case numbers of all viral diseases markedly decreased in both countries; however, bacterial gastrointestinal infectious diseases showed a different pattern.
-
CONCLUSIONS
- The incidence of gastrointestinal infectious diseases decreased after the COVID-19 outbreak. In contrast, Campylobacter infections showed an increasing trend in Korea, but a decreasing trend in the United States. Further studies are needed to elucidate the different trends in bacterial and viral infectious diseases before and after non-pharmaceutical interventions and between different countries.
- On March 11, 2020, the World Health Organization (WHO) declared coronavirus disease 2019 (COVID-19) as a pandemic. After the WHO declaration, non-pharmacological interventions (NPIs) against COVID-19 were implemented in several countries [1]. NPIs such as movement restrictions and isolation measures began in March 2020 worldwide [2], and Korea also started implementing nationwide NPIs in March 2020 [3,4]. As a result of NPIs, the weekly positivity rates of viral respiratory infections significantly decreased in 2020 compared with those in the same weeks in 2010-2019 [5]. Interventions, including personal hygiene and social distancing measures, might affect infectious diseases other than respiratory infectious diseases. However, whether NPIs could influence the development of other infectious diseases is unknown owing to the limited number of studies. Therefore, we examined how trends in the weekly frequencies of gastrointestinal infectious diseases changed before and during the COVID-19 pandemic in Korea, considering trends in COVID-19 incidence, and compared them with the trends in the United States.
INTRODUCTION
- We analyzed the weekly number of cases of gastrointestinal infectious diseases from the Infectious Disease Surveillance System established by the Korea Disease Control and Prevention Agency (KDCA; formerly the Korea Centers for Disease Control and Prevention). Physicians reported cases to this surveillance system based on the Infectious Disease Control and Prevention Act [6]. After collecting data from the local health authorities, these data were transferred to the KDCA. A report of national statistics was then published using confirmed data from the KDCA [7]. According to reporting guidelines, reported infectious diseases are classified into 3 groups; pathogen identified, suspected infection, or a pathogen carrier [8]. The infectious disease surveillance system in Korea is composed of a mandatory surveillance system and a sentinel surveillance system [6,9]. The mandatory surveillance system requires obligatory reporting from all health centers immediately or within 24 hours of identifying 64 types of infectious diseases. The sentinel surveillance system receives weekly reports on 23 types of infectious diseases from designated health institutions. In this study, we considered gastrointestinal infectious diseases, including cholera, shigellosis, typhoid, paratyphoid, enterohemorrhagic Escherichia coli (EHEC), and hepatitis A virus, which are collected through the mandatory surveillance system: Salmonella, enteroinvasive E. coli (EIEC), Yersinia enterocolitica, Clostridium perfringens, Vibrio parahaemolyticus, enteropathogenic E. coli (EPEC), Bacillus cereus, Campylobacter, enterotoxigenic E. coli (ETEC), Listeria monocytogenes, Staphylococcus aureus, group A rotavirus, astrovirus, adenovirus, norovirus, and sapovirus infections, which are collected through the sentinel surveillance system [9]. For a cross-country comparison with the United States, we used weekly reports from the Nationally Notifiable Diseases Surveillance System (NNDSS) administered by the United States Centers for Disease Control and Prevention (CDC) [10], to which infectious and contagious diseases are immediately reported by healthcare providers [11,12]. The NNDSS is collected from all 50 states and the District of Columbia and monitors about 120 diseases classified by the main transmission: sexually transmitted, foodborne or waterborne, vector borne, injection drug use–associated, and respiratory [13]. As a result, the types of infectious agents reported in the KDCA in Korea and the CDC in the United States differed. Thus, we selected infectious diseases from the CDC that overlapped with those in the KDCA for comparison: salmonellosis, Campylobacter infection, typhoid, shigellosis, and hepatitis A virus infection. For the period before COVID-19, the mandatory surveillance system used the mean weekly number of cases from 2015 to 2019, which was calculated as the sum of all weekly case numbers divided by 5 (the number of years). The sentinel surveillance system used data from July 30, 2017 to 2019, considering the expansion of medical centers for sentinel surveillance in July 2017. For the period after COVID-19, we used the weekly number of cases of each type of gastrointestinal infectious disease from weeks 5-52 of 2020. We then compared the mean weekly case number for the same weeks before and after COVID-19 in the mandatory surveillance system and the sentinel surveillance system using the paired t-test.
- We excluded 1-4 weeks from each year to reflect the incidence of COVID-19 because the first COVID-19 patient was identified in Korea on January 20, 2020. Data on the number of weekly COVID-19 cases from the CDC in the United States [14] and from the KDCA in Korea [3] were used. For visualization, we plotted the trends in the weekly number of new COVID-19 cases together with the mean weekly number of each gastrointestinal infectious disease for 2 periods (before and after COVID-19). All statistical analyses were conducted using Microsoft Excel (version 2016; Microsoft, Redmond, WA, USA).
- Ethics statement
- This study used from official websites which are opened to the public. In accordance with Article 13 of the Enforcement Ordinance, this study is subject to institutional review board exception.
MATERIALS AND METHODS
- Table 1 shows the mean weekly number of cases of gastrointestinal infectious diseases during weeks 5-52 before COVID-19 compared with that after COVID-19 in Korea and the United States. In Korea, the weekly case number of total gastrointestinal infectious diseases showed a significant decrease (from 522 before COVID-19 to 245 after COVID-19, p< 0.01). Statistically significant decreases were observed for all types of viral gastrointestinal infectious diseases (range of decrease: -55.2 to -5.8, p< 0.01). The decreases for total bacterial gastrointestinal infectious diseases were not statistically significant (p= 0.12). In contrast, the number of total viral gastrointestinal infectious diseases markedly decreased after COVID-19 compared with the period before COVID-19. Meanwhile, in the United States, the number of cases significantly decreased for both total bacterial gastrointestinal diseases and total viral gastrointestinal diseases. In particular, in Korea, statistically significant decreases were observed for Salmonella, V. parahaemolyticus, ETEC, EIEC, S. aureus, B. cereus, typhoid, and shigellosis. A statistically significant increase was observed for Campylobacter infections. There were no statistically significant differences in C. perfringens, Y. enterocolitica, Listeria monocytogenes, EHEC, cholera, paratyphoid, and EPEC infections. In the United States, significant decreases were found for salmonellosis (-151.8), Campylobacter infection (-163.9), typhoid (-1.5), shigellosis (-71.9), and hepatitis A virus infection (-15.5) after COVID-19 compared before COVID-19 (p< 0.01 for all).
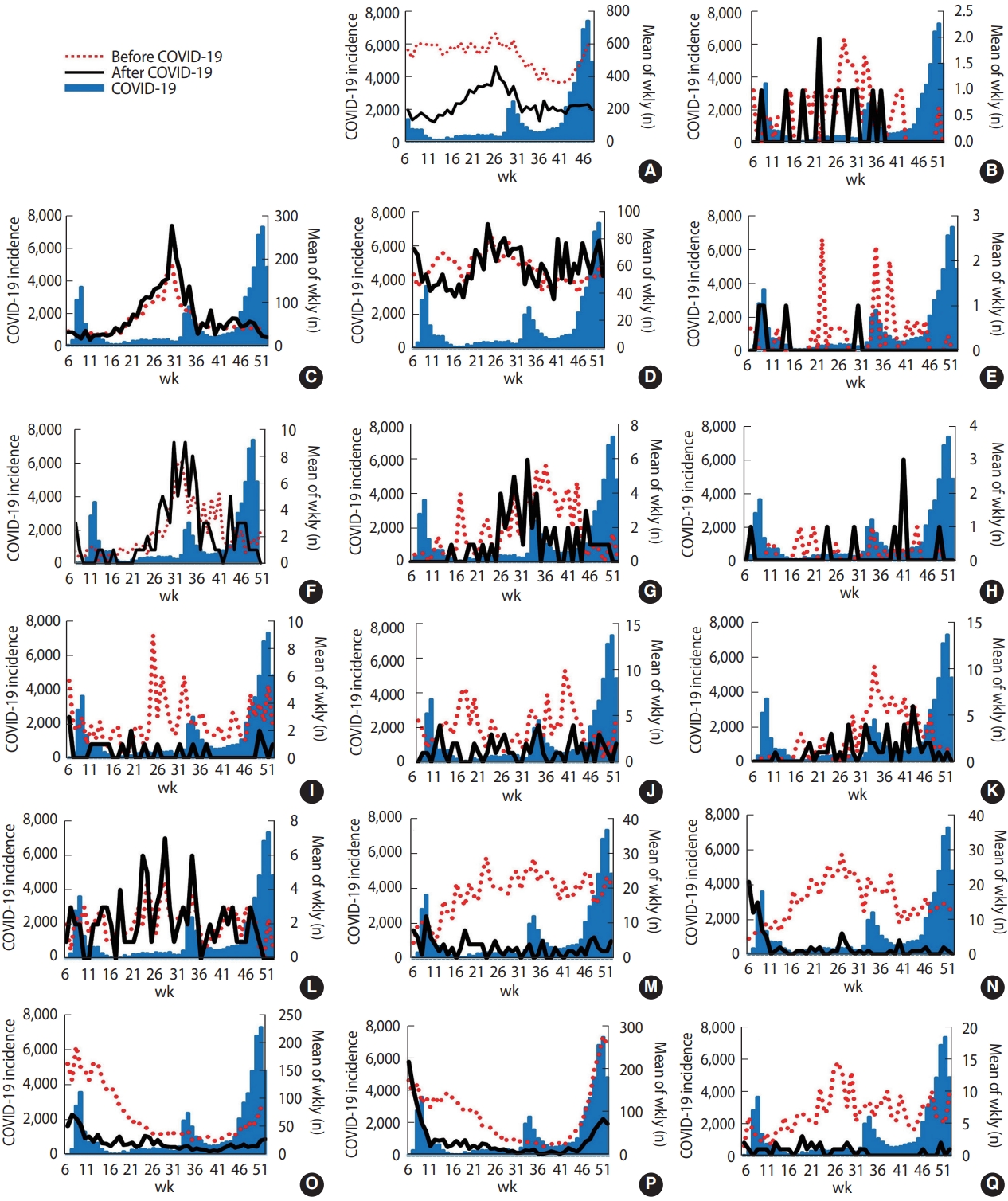
- Figures 1 and 2 present the epidemic curves of each type of gastrointestinal infectious disease determined by sentinel surveillance and mandatory surveillance during weeks 5–52 before and after COVID-19 in Korea with the weekly number of new COVID-19 cases. After the start of the COVID-19 outbreak, followed by the establishment of NPIs in Korea, the frequency of the 6 types of viral diseases decreased, especially group A rotavirus, astrovirus, adenovirus, norovirus, and sapovirus infections. In particular, the frequency of astrovirus and sapovirus infections reached nearly 0 from week 41. The epidemic patterns of bacterial diseases did not show a dramatic decrease after COVID-19.
- Figure 3 shows that the weekly case numbers of Salmonella infection, Campylobacter infection, typhoid, shigellosis, and hepatitis A virus infection sharply decreased after the COVID-19 outbreak in the United States. The decrease in the number of shigellosis cases was most pronounced, from 124 on week 9 to 9 on week 18.
RESULTS
- With respect to the 5 gastrointestinal infections that were collected in both countries, not only the weekly case numbers of each bacterial and viral disease, but also the total case number of bacterial and viral gastrointestinal diseases markedly decreased in the United States. However, Korea showed a different pattern. Specifically, the total number of viral gastrointestinal diseases decreased significantly, while the total number of bacterial gastrointestinal diseases did not significantly decrease. In addition, each bacterial gastrointestinal disease had distinct trends.
- Infectious diseases are expected to decrease after the COVID-19 pandemic due to worldwide NPIs. In Korea, the total number of viral gastrointestinal infections showed a considerable decrease, but the decreases in the total bacterial gastrointestinal infections did not reach a statistically significant level. Unlike the viral gastrointestinal infectious diseases, there were fluctuations in the trends of bacterial gastrointestinal infections (downward, stable, and then upward) in 2020 compared with previous years. Significant decreases were observed for Salmonella, V. parahaemolyticus, ETEC, EIEC, S. aureus, B. cereus, typhoid, and shigellosis. However, only the increase in Campylobacter infections was statistically significant. NPIs, such as hand hygiene and wearing a mask, can reduce the spread of viral diseases [15], and these viral gastrointestinal infectious diseases also showed a significant decrease like that observed for respiratory viruses, suggesting the existence of a foodborne or waterborne infection route for gastrointestinal viruses [16,17]. However, C. perfringens and EHEC did not show significant increases. This finding was probably due to an unstable small number. In the case of EHEC, the outbreak in 2019 may have affected the increase in EHEC [18]. Bacterial gastrointestinal infections were difficult to identify both before and after the COVID-19 outbreak. Bacterial pathogens propagate through rotten food or water, especially during the summer [19,20].
- Since the types of gastrointestinal infections collected in Korea and the United States differed, the possibility of a direct comparison would be limited; however, there are several potential reasons for the observed divergence. First, the United States issued stay-athome orders between March and April 2020. In Korea, personal hygiene measures, such as mask-wearing, were used. Second, compared to the United States, Korea implemented a less strict social distancing policy, and therefore, accessibility to medical care may have been lower in the United States than in Korea [7]. Consequently, people who had gastrointestinal infectious diseases with less severe symptoms might have had a limited ability to access medical centers during the COVID-19 pandemic than during the period before it, which could have had a greater impact in the United States than in Korea. Thus, despite the possibility of underreporting followed by underestimation of actual infection numbers in both countries, this would be more impactful in the United States [21]. Despite these potential reasons, Campylobacter infections showed clearly different patterns between Korea and the United States. Gastrointestinal infectious diseases have a wide range of infection pathways. The agents of Campylobacter infections are animals, including dogs, cats, pigs, sheep, rodents, birds, and poultry [9]. According to a Korean study, retail raw chickens were confirmed in about 68% of cases for Campylobacter. After the COVID-19 outbreak, the annual consumption of chicken per adult increased by 1.2 kg compared to COVID-19 [22]. Thus, Campylobacter infections are a zoonotic contagious disease that can infect humans through food based on these assumptions. Additionally, in Korea, cluster outbreaks in restaurants accounted for the highest number of cases before COVID-19; however, after COVID-19, the most common place of cluster outbreaks shifted to pre-primary schools [9]. In Korea, kindergartens and pre-primary schools have different purposes. Kindergartens focus on education, and pre-primary schools focus on childcare. Therefore, this could explain the poor control of Campylobacter in the context of COVID-19. Our data, including the mandatory surveillance and sentinel surveillance, and, in the case of sentinel surveillance, the number of hospitals (including public hospitals) collecting data, increased from July 30, 2017 [23]. Thus, we compared the periods before and after COVID-19 separately for each surveillance system.
- In conclusion, while the incidence of viral gastrointestinal diseases, including hepatitis A, prominently decreased after COVID-19, bacterial diseases showed different trends in Korea and a decreasing trend in the United States. Further studies are needed to elucidate the different trends in bacterial and viral infectious diseases before and after NPIs and between different countries, as well as considering the characteristics of each pathogen.
DISCUSSION
-
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare for this study.
-
FUNDING
This research was supported by the Government-wide R&D Fund Project for Infectious Disease Research (GFID), Republic of Korea (grant No. HG18C00880).
This study was conducted under the research project “Research and Development on Integrated Surveillance System for Early Warning of Infectious Diseases” (RISEWIDs).
-
AUTHOR CONTRIBUTIONS
Conceptualization: Park B, Kim S. Data curation: Kim S, Kim J. Formal analysis: Kim S. Funding acquisition: Choi BY. Methodology: Park B, Kim S. Project administration: Park B, Choi BY. Visualization: Kim S. Writing – original draft: Kim S, Kim J, Park B. Writing – review & editing: Kim S, Park B, Choi BY.
NOTES
ACKNOWLEDGEMENTS



| Variables |
Korea |
United States |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Before COVID-19 | After COVID-19 | Difference | p-value | Before COVID-19 | After COVID-19 | Difference | p-value | |||
| Total no. of gastrointestinal infectious diseases | 522.1±83.3 | 245.0±98.2 | -277.1 | <0.01 | 1,021.0±257.0 | 616.0±205.0 | -405 | <0.01 | ||
| Bacterial | ||||||||||
| Total | 190.7±70.8 | 182.0±91.6 | -8.7 | 0.12 | 965.5±252.5 | 576.2±193.6 | -389.3 | <0.01 | ||
| Sentinel surveillance1 | ||||||||||
| Salmonella | 52.4±32.2 | 38.0±27.2 | -14.4 | <0.01 | 350.8±132.9 | 199.0±94.1 | -151.8 | <0.01 | ||
| Vibrio parahaemolyticus | 2.6±2.6 | 1.0±1.4 | -1.6 | <0.01 | - | - | - | - | ||
| Enterotoxigenic Escherichia coli | 1.8±1.6 | 1.0±1.4 | -0.8 | <0.01 | - | - | - | - | ||
| Enteroinvasive Escherichia coli | 0.3±0.6 | 0.1±0.3 | -0.2 | 0.02 | - | - | - | - | ||
| Campylobacter | 57.1±38.3 | 67.0±55.1 | 9.9 | <0.01 | 497.3±126.4 | 333.4±104.5 | -163.9 | <0.01 | ||
| Clostridium perfringens | 57.9±9.9 | 59.0±13.9 | 1.1 | 0.35 | - | - | - | - | ||
| Staphylococcus aureus | 3.7±2.2 | 1.0±1.2 | -2.7 | <0.01 | - | - | - | - | ||
| Bacillus cereus | 0.6±0.6 | 0.2±0.5 | -0.4 | <0.01 | - | - | - | - | ||
| Yersinia enterocolitica | 2.2±1.0 | 2.0±1.6 | -0.2 | 0.73 | - | - | - | - | ||
| Listeria monocytogenes | 0.2±0.3 | 0.1±0.5 | -0.1 | 0.84 | - | - | - | - | ||
| Enteropathogenic Escherichia coli | 2.3±1.9 | 2.0±2.5 | -0.3 | 0.60 | - | - | - | - | ||
| Mandatory surveillance2 | ||||||||||
| Cholera | 0.1±0.1 | 0.1±0.1 | -0.1 | 0.15 | - | - | - | - | ||
| Typhoid | 2.6±1.1 | 0.7±0.9 | -1.8 | <0.01 | 2.1±1.0 | 0.6±0.9 | -1.5 | <0.01 | ||
| Paratyphoid | 1.1±0.6 | 1.1±1.3 | 0.0 | 0.88 | - | - | - | - | ||
| Shigellosis | 2.4±1.1 | 0.4±0.7 | -2.0 | <0.01 | 115.2±13.7 | 43.3±29.0 | -71.9 | <0.01 | ||
| Enterohemorrhagic Escherichia coli | 2.7±1.9 | 5.5±10.8 | 2.8 | 0.06 | - | - | - | - | ||
| Viral | ||||||||||
| Total | 371.3±87.9 | 147.7±80.1 | -223.6 | <0.01 | 54.6±10.9 | 39.1±18.4 | -15.5 | <0.01 | ||
| Sentinel surveillance1 | ||||||||||
| Group A rotaviruses | 73.0±48.3 | 23.0±16.8 | -50.0 | <0.01 | - | - | - | - | ||
| Astrovirus | 15.4±6.0 | 2.0±5.1 | -13.4 | <0.01 | - | - | - | - | ||
| Adenovirus | 18.5±6.0 | 3.0±2.6 | -15.5 | <0.01 | - | - | - | - | ||
| Norovirus | 95.2±66.1 | 40.0±59.5 | -55.2 | <0.01 | - | - | - | - | ||
| Sapovirus | 6.5±3.0 | 0.7±1.0 | -5.8 | <0.01 | - | - | - | - | ||
| Mandatory surveillance2 | ||||||||||
| Hepatitis A | 124.0±42.4 | 77.6±17.0 | -46.3 | <0.01 | 54.6±10.9 | 39.1±18.4 | -15.5 | <0.01 | ||
Values are presented as mean weekly number±standard deviation.
1 The weekly number of each type of gastrointestinal infectious disease in weeks 5-52 of 2020 with the mean of the same weeks during July 30, 2017-2019 in Korea or during 2015-2019 in United States.
2 The weekly number of each type of gastrointestinal infectious disease in weeks 5-52 of 2020 with the mean of the same weeks during 2015-2019 in Korea and United States.
- 1. World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19 - 30 March 2020 [cited 2021 Jun 10]. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---30-march-2020.
- 2. Askitas N, Tatsiramos K, Verheyden B. Estimating worldwide effects of non-pharmaceutical interventions on COVID-19 incidence and population mobility patterns using a multiple-event study. Sci Rep 2021;11:1972.ArticlePubMedPMC
- 3. Korea Disease Control and Prevention Agency. Coronavirus (COVID-19), Republic of Korea [cited 2020 Jun 11]. Available from: http://ncov.mohw.go.kr/en.
- 4. Dighe A, Cattarino L, Cuomo-Dannenburg G, Skarp J, Imai N, Bhatia S, et al. Response to COVID-19 in South Korea and implications for lifting stringent interventions. BMC Med 2020;18:321.ArticlePubMedPMC
- 5. Yum S, Hong K, Sohn S, Kim J, Chun BC. Trends in viral respiratory infections during COVID-19 pandemic, South Korea. Emerg Infect Dis 2021;27:1685-1688.ArticlePubMedPMC
- 6. Korea Ministry of Government Legislation. Infectious Disease Control and Prevention Act [cited 2021 Nov 22]. Available from: http://law.go.kr/ (Korean).
- 7. Park S, Cho E. National infectious diseases surveillance data of South Korea. Epidemiol Health 2014;36:e2014030.ArticlePubMedPMC
- 8. Park M. Infectious disease-related laws: prevention and control measures. Epidemiol Health 2017;39:e2017033.ArticlePubMedPMC
- 9. Korea Disease Control and Prevention Agency. Infectious disease portal [cited 2021 Jun 10]. Available from: https://www.kdca.go.kr/npt/biz/npp/nppMain.do (Korean).
- 10. Centers for Disease Control and Prevention. Notifiable infectious disease data tables; 2021 [cited 2021 Jun 10]. Available from: https://www.cdc.gov/nndss/data-statistics/infectious-tables/index.html.
- 11. Troppy S, Haney G, Cocoros N, Cranston K, DeMaria A Jr. Infectious disease surveillance in the 21st century: an integrated web-based surveillance and case management system. Public Health Rep 2014;129:132-138.ArticlePubMedPMC
- 12. Adams DA, Jajosky RA, Ajani U, Kriseman J, Sharp P, Onwen DH, et al. Summary of notifiable diseases--United States, 2012. MMWR Morb Mortal Wkly Rep 2014;61:1-121.PubMed
- 13. Crane MA, Popovic A, Panaparambil R, Stolbach AI, Romley JA, Ghanem KG. Reporting of infectious diseases in the United States during the COVID-19 pandemic. Clin Infect Dis 2021;ciab529.
- 14. CDC COVID-19 Response Team. Coronavirus disease 2019 in children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep 2020;69:422-426.ArticlePubMedPMC
- 15. Laszkowska M, Kim J, Faye AS, Joelson AM, Ingram M, Truong H, et al. Prevalence of Clostridioides difficile and other gastrointestinal pathogens in patients with COVID-19. Dig Dis Sci 2021;66:4398-4405.ArticlePubMedPMC
- 16. Matsuyama R, Miura F, Nishiura H. The transmissibility of noroviruses: statistical modeling of outbreak events with known route of transmission in Japan. PLoS One 2017;12:e0173996.ArticlePubMedPMC
- 17. Matsuyama R, Miura F, Tsuzuki S, Nishiura H. Household transmission of acute gastroenteritis during the winter season in Japan. J Int Med Res 2018;46:2866-2874.ArticlePubMedPMC
- 18. Lee SH, Yun JW, Lee JH, Jung YH, Lee DH. Trends in recent waterborne and foodborne disease outbreaks in South Korea, 2015-2019. Osong Public Health Res Perspect 2021;12:73-79.ArticlePubMedPMC
- 19. Wen SC, Best E, Nourse C. Non-typhoidal Salmonella infections in children: review of literature and recommendations for management. J Paediatr Child Health 2017;53:936-941.ArticlePubMed
- 20. Kim JS, Lee MS, Kim JH. Recent updates on outbreaks of Shiga toxin-producing Escherichia coli and its potential reservoirs. Front Cell Infect Microbiol 2020;10:273.ArticlePubMedPMC
- 21. Kang HY, Shin E, Kim YS, Kim JK. Comparing physicians’ reporting propensity with active and passive surveillance systems in South Korea. J Korean Med Assoc 2014;57:167-175.Article
- 22. Han K, Jang SS, Choo E, Heu S, Ryu S. Prevalence, genetic diversity, and antibiotic resistance patterns of Campylobacter jejuni from retail raw chickens in Korea. Int J Food Microbiol 2007;114:50-59.ArticlePubMed
- 23. Korea Disease Control and Prevention Agency. Guideline for water & foodborne diseases prevention and control 2022 [cited 2021 Jun 10]. Available from: https://www.kdca.go.kr/npt/biz/npp/portal/nppPblctDtaView.do?pblctDtaSeAt=8&pblctDtaSn=2567 (Korean).
REFERENCES
Figure & Data
References
Citations
- Trends in Nationally Notifiable Infectious Diseases in Humans and Animals during COVID-19 Pandemic, South Korea
Taehee Chang, Sung-il Cho, Dae sung Yoo, Kyung-Duk Min
Emerging Infectious Diseases.2024;[Epub] CrossRef - Impact of the COVID‐19 pandemic on the circulation of other pathogens in England
Lauren J. Hayes, Hannah Uri, Denisa Bojkova, Jindrich Cinatl, Mark N. Wass, Martin Michaelis
Journal of Medical Virology.2023;[Epub] CrossRef - Understanding the impact of the COVID-19 pandemic response on GI infection surveillance trends in England, January 2020–April 2022
Nicola K. Love, Amy Douglas, Saheer Gharbia, Helen Hughes, Roger Morbey, Isabel Oliver, Gillian E. Smith, Alex J. Elliot
Epidemiology and Infection.2023;[Epub] CrossRef - Trends for Syndromic Surveillance of Norovirus in Emergency Department Data Based on Chief Complaints
Soyeoun Kim, Sohee Kim, Bo Youl Choi, Boyoung Park
The Journal of Infectious Diseases.2023;[Epub] CrossRef - Trends in Gastrointestinal Infections during the COVID-19 Pandemic and Concerns of Post-Pandemic Resurgence in Japan
Takuma Higurashi, Shigeki Tamura, Noboru Misawa, Nobuyuki Horita
Diseases.2023; 12(1): 4. CrossRef - Characteristics and related factors of waterborne and foodborne infectious disease outbreaks before and after the onset of the COVID-19 pandemic (2017–2021) in the Republic of Korea: a descriptive study
Eunkyoung Kim, Bryan Inho Kim
Osong Public Health and Research Perspectives.2023; 14(6): 483. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite




