A systematic review of barriers and motivators to physical activity in elderly adults in Iran and worldwide
Article information

Abstract
OBJECTIVES
This study was conducted to identify and characterize the barriers and motivations to physical activity (PA) for elderly adults in Iran and other countries.
METHODS
We searched 6 databases (PubMed, Embase, Scopus, Web of Science, Magiran, and the Scientific Information Database) from 2000 to the November 2017, using “aged 60 and over,” “physical activity” or “exercise,” and “motivator” and “barrier” as keywords. Two reviewers independently performed the search, screening, and quality assessment of the studies.
RESULTS
In total, 34 papers were finally included in the study. The most important barriers, based on the frequency of factors, included physical problems, having no companions, and physical barriers to walking. The motivators included improving one’s physical condition, being social, and suitability of the physical environment.
CONCLUSIONS
Important motivators and barriers to PA were more closely related to intrapersonal factors than to the interpersonal and environmental domains. The barriers and motivators to PA in the elderly were not markedly different between Iran and other countries. Therefore, a general strategy could be designed to improve PA in the elderly.
INTRODUCTION
On one hand, physical activity (PA) helps elderly people to improve their strength and flexibility, although the most effective type of activity is still unclear [1]. On the other hand, the elderly—due to health problems and insufficient facilities—are more likely to face barriers to access than others [2].
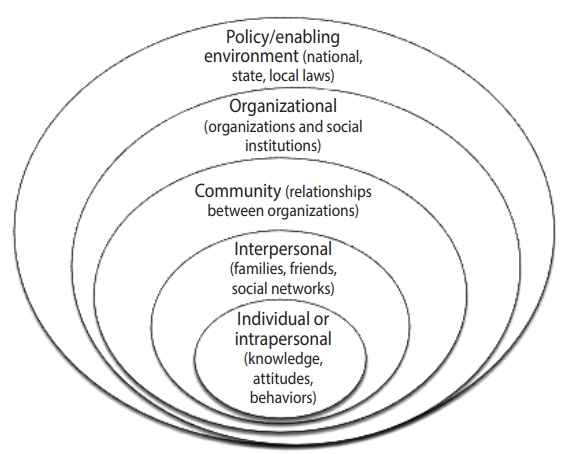
For adults aged 60 and over, important motivations for PA have been reported to include social support, health benefits, and enjoyment, while the main barriers have been found to be insufficient guidance and a lack of role models [3]. For people aged over 80 years, the most important motivators and barriers have been reported to be the health benefits of PA, various types of fears, individual preferences, and social support [4]. In general, due to the increasing percentage of the older population in developing (low-and middle-income) countries and the burden of health care and treatment costs, reducing the prevalence of physical inactivity has received attention as an important goal [5]. In addition, PA develops as a behavior through complex and dynamic interrelations among individual, social, and environmental factors, underscoring the usefulness of using multidimensional models to study PA [6,7]. As an example of this approach, the socio-ecological model of McLeroy et al. [8] was used to study the barriers and motivations to PA in the elderly. The aim of this study was to systematically review the motivators and barriers to PA in people aged 60 years and older in Iran and other countries.
MATERIALS AND METHODS
Search strategy
To collect the data, a comprehensive search was performed of several electronic databases (PubMed [MeSH terms], Web of Science, Scopus, Embase, Scientific Information Database, Magiran) to identify all potentially relevant publications in the Persian and English languages from 2000 to November 2017. The following keywords were used: “aged (or age 60 and over),” “physical activity (or exercise),” and “motivator and barrier” (Supplementary Material 1). The detailed search strategy implementation in PubMed was as follows: ([elderly OR Aged OR “60 over aged”] AND [“Physical activity” OR “Exercise” OR “Physical exercise” OR “Motor activity”] AND [Motivation OR Motivat* OR Barrier*]). The inclusion criteria were (1) articles published in the Persian and English languages; (2) original research examining the barriers and motivators to PA in the elderly; (3) studies that examined outcomes in terms of physical and mental illness among the elderly (aged 60 and over); and (4) studies conducted from from 2000 to November 2017. The exclusion criteria were non-original articles (i.e., letters to the editor, case reports, interventional studies, reviews, meta-analyses, and articles presented at seminars and conferences were excluded), articles with no specific definition of age, those that were conducted before 2000 but were accepted in 2000 or later, articles analyzing elderly individuals living in nursing homes, and articles with a very low quality score. In addition, a backward search (checking bibliographic mining of identified papers for any additional studies) was conducted to identify any studies that were not retrieved using the main search strategy. All quantitative and qualitative designs were included. In total, 1,981 articles were retrieved, of which a total of 34 articles remained after the review process shown in Figure 1. Finally, 2 authors carefully examined 34 full-text articles.

The literature review and retrieval process.
In this study, 2 types of studies were investigated: (1) quantitative studies (5 from Iran and 15 from other countries); (2) qualitative studies (1 from Iran and 13 from other countries).
There were 6 studies in Persian and 28 studies in English.
Evaluating the quality of articles
The quality of qualitative studies was assessed using the qualitative methodological checklist of the National Institute of Clinical Nursing (NICE) [9]. In general, according to the NICE checklist, ++ means that all or most of the checklist criteria have been fulfilled, + means that some of the checklist criteria have been fulfilled, and – means that few or no checklist criteria have been fulfilled. Quantitative studies were assessed using the Newcastle-Ottawa Quality Assessment Scale (NOS) adapted for cross-sectional studies [10]. The NOS is based on 3 domains, including the selection of study groups, the comparability of groups, and the description of exposures and outcomes. This scale, which includes 8 items is scored in terms of stars, assesses the quality of each study in each domain. All items except the comparability domain have 1 star, while the maximum score for the comparability domain is 2 stars. The total number of earned stars is calculated as the total quality score for each study, which ranges from 1 star (very poor) to 10 stars (high quality). Studies were classified as high-quality (8-10), medium-quality (6-7), or low-quality (<6). Two review authors (SY and HMS) completed the quality assessment independently. In cases of disagreement or items that remained unclear, a third review author (AR or MG) was consulted.
Data extraction
We used a structured form to extract the data. The extracted data included study and participant characteristics (e.g., gender, location, country, population, age, type of instrument, type of study, year of study), as well as motivators and barriers to PA. Two authors (SY and HMS), who conducted the study selection independently, performed the data extraction. Any disagreements were discussed with a third review author (AR or MG) if necessary. The data were classified using the socio-ecological model that McLeroy et al. [8] developed in 1988 as a theoretical framework involving interpersonal and intrapersonal factors, organizational and social factors, and environmental factors (Figure 2). The identified factors were prioritized based on the frequency of participants’ responses.
Ethics statement
This study is a systematic review and does not deal with human participants.
RESULTS
Quality of qualitative and quantitative studies
Fortunately, almost all the qualitative studies followed the items in the NICE checklist for qualitative studies. Two of the 14 qualitative articles were high-quality, 12 were good-quality, and 5 were poor-quality, as indicated in Table 1. The quantitative studies were evaluated using the NOS scale, and 18 articles were found to be moderate- to high-quality, while 2 were moderate-quality.
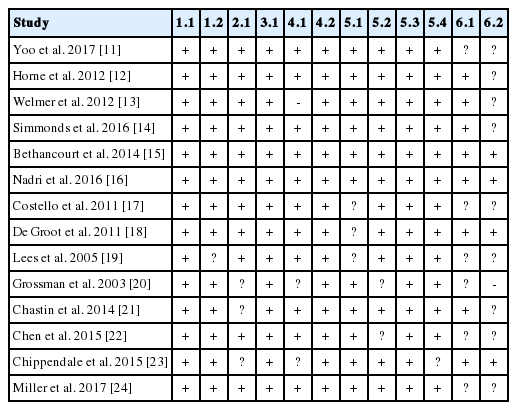
Quality assessment of qualitative articles
Description of reviewed studies
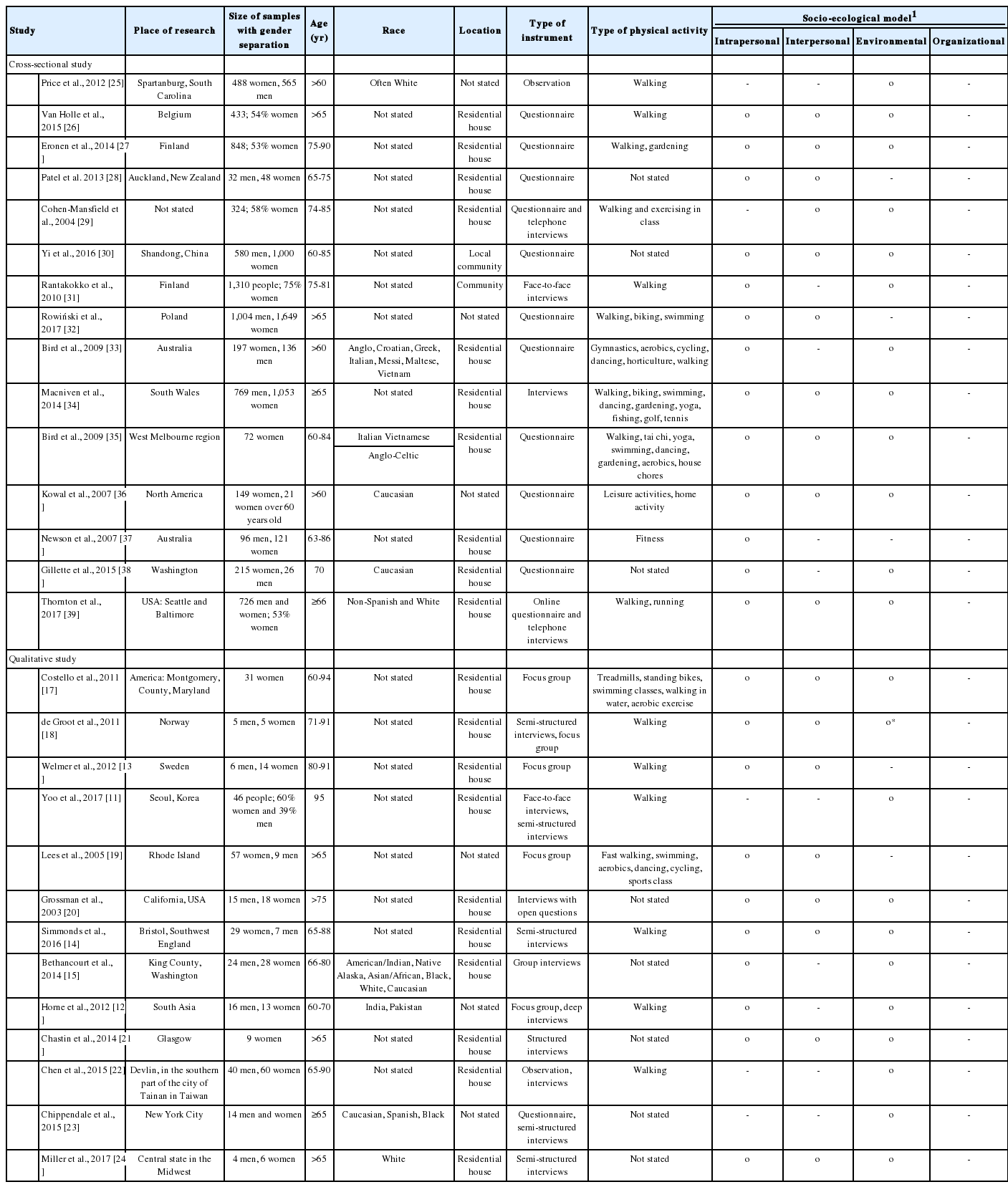
The articles were published between 2000 and November 2017, and the sample sizes ranged from 9 (in a qualitative study) to 4,227 participants (in a quantitative study). The samples consisted of both men and women subjects in 30 of the 34 studies, exclusively of women subjects in 4 studies, and exclusively of men subjects in 1 study. The most common type of PA was walking, followed by swimming and fitness, and a description of the type of PA was not available in 17 studies.
In Tables 2 and 3, the characteristics and major findings of the studies are presented.
Description of the findings reported in eligible studies
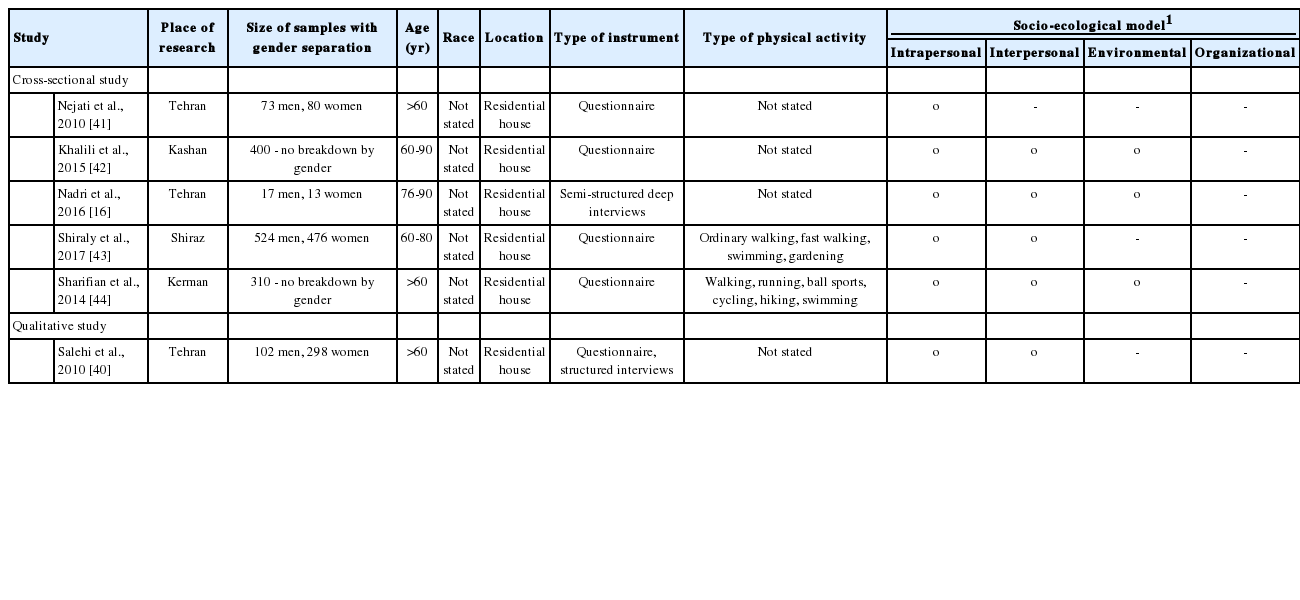
Description of the findings reported in eligible Iranian studies
Motivators and barriers to the physical activity among the elderly
In the framework of the McLeroy model, we examined the motivators and barriers to PA among the elderly in the intrapersonal, interpersonal, and environmental domains as follows (Tables 2 and 3). According to the study population—people aged 60 years and older—the items from the organizational domain of the McLeroy model were excluded. For quantitative studies, only significant variables were evaluated. Due to the heterogeneity across studies and input variables, it was not possible to conduct a meta-analysis of the results. Below, the most important factors for all dimensions of the model, based on the frequency of participants’ responses, are presented.
Intrapersonal factors
Through the literature review, 23 barriers and 16 motivators were identified as intrapersonal factors. In several articles, physical problems—such as difficulty in walking, physical health problems, physical weakness, respiratory problems, and lack of energy—were mentioned as key barriers [13,14,16,19,27,31-34,36, 38-41,43-45]. Time limits were the second most important barrier related to intrapersonal factors [16,17,19,27,28,35,36,39,42-44]. The third most important intrapersonal barrier was fear of falling [14,17,19,23,27,31,35,40,43,45].
The most important intrapersonal set of motivators that resulted in PA was improving one’s physical condition, which included improving one’s balance and walking ability, reducing muscle pain, improving sleep, and strengthening one’s muscles [18,24,34,41,44]. Enjoyment [12,24,40,44], addressing psychological issues (which involved relief from stress, feeling more efficient, having positive perceptions of PA, having a positive self-image, being less depressed, and enhancing sleep [14,16,33,41]), and increasing motivation and access to PA resources [15,30,34,38] comprised the second most important set of intrapersonal motivators [12,24,28,40,44,45]. The third most important set of intrapersonal motivators included a lack of knowledge [17,30], health concerns [17,37], and being economical [24,34].
Interpersonal factors
In the interpersonal domain, 6 barriers and 7 motivations were identified (Table 4). The most important interpersonal barrier to PA was having no companion [36,42]. Family responsibilities (taking care of grandchildren, children, and sick people at home) were the second most important interpersonal barrier to PA [34].
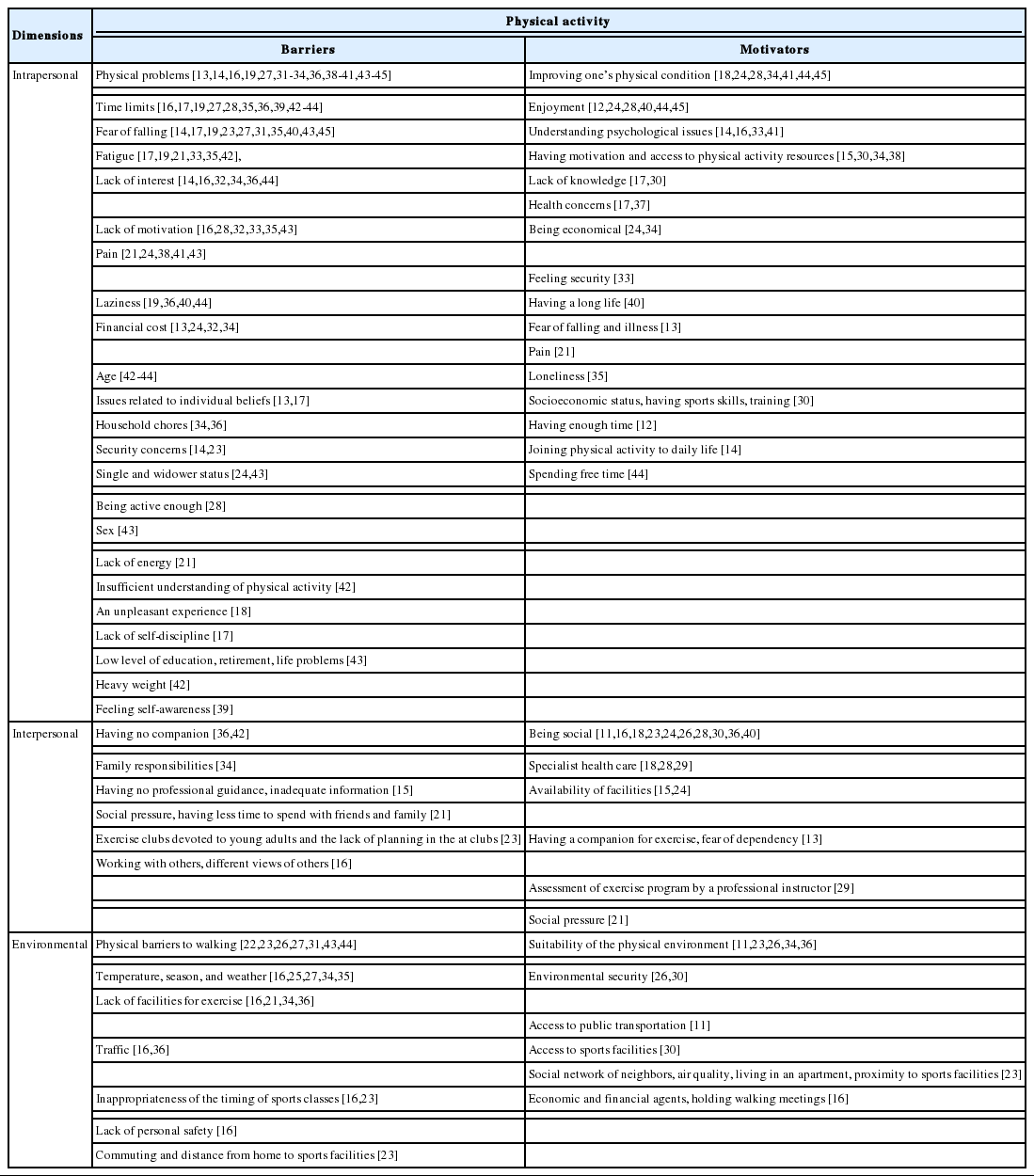
Motivations and barriers to physical activity for the elderly
The most important interpersonal motivator was being social, which included communication with friends, peer support, communication with others, exercise with friends, social coherence, moderate and high local dependency, an abundance of companions for walking, and support from others [11,16,18,23,24,26,28,30,36,40]. Supervision of health professionals was the second interpersonal motivator [18,28,29]. In addition, 3 articles identified specialist health care [18,28,29] as a motivator for PA. Another important interpersonal motivator for PA was the availability of sports facilities [15,24].
Environmental factors
Overall, 7 barriers and 6 motivators were identified at the community level. The most important barrier was physical barriers to walking, which included problems related to safety, parked motorcycles next to the street, potted plants, rubber tiles in playgrounds, food retailers, paved streets, broken sidewalks, scaffolds, snow accumulation along the street in winter, devoted seats in parks for children, the lack of facilities such as benches for resting, poor locations, unsafe roads, stray dogs, and hills [22,23,26,27,31,43,44]. The second most important set of barriers were related to temperature, season, and weather [16,25,27,34,35]. More intense PA among the elderly was observed in the spring (40.1%), in sunny weather (76.8%), and at moderate temperatures (56.2%) [25]. The third most important barrier was a lack of facilities for exercise [16,21,34,36].
The most important environmental motivator was the suitability of the physical environment. This factor included pleasant landscapes, streetlights, sidewalks, bike riding routes, walking paths, the neighborhood’s suitability for walking, interconnections between streets and an attractive environment, an environment free from non-cultural social activities (e.g., smoking, drinking alcohol, gambling), green space, attractive architecture, benches for resting, a place for dog parks, a smooth surface for hiking, and food availability in urban centers [11,23,26,34,36]. Environmental security was the second environmental motivator [26,30].
DISCUSSION
In the present study, information on PA among the elderly was reviewed from 2000 to November 2017. We aimed to identify the motivators and barriers to PA among individuals aged over 60 in Iran and worldwide; therefore, some studies were excluded because they did not analyze participants under or over 60 years of age as 2 different groups [2,36]. In general, the ecological model is a comprehensive multilevel framework that includes contributors to active behavior at all levels: individual (interpersonal and intrapersonal), social, environmental, and policy [47].
A systematic review by Baert et al. [4] on adults aged over 79 confirmed that quantitative research has a greater focus on the interpersonal and community levels, while qualitative research tends to focus more on the interpersonal level. We found that more research is needed into barriers and motivators at the organizational level, while Baert et al. [4] showed that community-based barriers and motivators need more research because policy-makers may be able to exert influence on these factors.
Intrapersonal factors
Health status was highlighted in most articles, either as a barrier (18 times) or as a motivator (5 times) for PA. To summarize, in the literature review, 23 articles reported that poor health was a relevant factor for PA among those aged 60 and over. Moreover, the beneficial effects of PA on health status (such as improving balance, improving walking ability, reducing muscle pain, improving sleep, and strengthening) are well established. In addition, Baert et al. [4] reported that health status was both a barrier and motivator. Nonetheless, health improvement has been reported as an important motivator, and research has highlighted that health benefits can be a major factor for promoting PA [17]. In this review, most studies were conducted in Iran and the USA. In these countries, special consideration should be given to the proportion of the young population in light of current barriers. For example, since Iran is a country with a young population, the proportion of the elderly in Iran is expected to peak in the next 50 years, and Iran will face similar challenges to Europe and the USA between 2040 and 2050 [48].
Fear emerged as a special barrier. Fear is a complex phenomenon that can occur in different situations (e.g., fear of walking at night in order to exercise outside the house). It can be related to health status, such as fear of injury or pain, fear of falling, and fear of being dependent on others. Lim & Taylor [49] reported that fear of falling was associated with inadequate levels of PA. Moreover, fear of falling was identified as a barrier to PA in different races, including African-Americans, Whites, and American Indians. In particular, American Indians were worried about falling when there was nobody to help them [50]. Furthermore, anxiety and fear of injury were mentioned as a barrier [19]. Health care providers should recognize this type of fear, and should consider it as an important barrier to be dealt with appropriately, if necessary.
In our study, time limits or lack of time was identified as a barrier. This barrier has also been described in other studies [4]. In a focus group study, lack of time among people aged over 65 was found to be a barrier to PA [19]. In many countries and cultures, the responsibilities of taking care of children and the home take up many hours in the day, with consequent negative effects on health behavior [51].
Enjoying PA was reported as a motivator, as in other studies. Factors related to enjoyment increase the pleasure experienced during PA, which depends on individual preferences (doing physical exercise in a group or enjoying the landscape). Fortunately, health care providers can provide support and guidance in this respect [4].
Interpersonal factors
As has been found for other age groups, being social was identified as a motivator. In general, social support was also reported as a motivational factor. However, elderly individuals need more social support than younger adults [4]. Unfortunately, elderly people are often single, causing them to be socially isolated [24]. Supervision by health professionals has an important impact on PA in the elderly; in particular, health care providers can encourage elderly people to participate in group exercises. It has been suggested that by providing information and raising awareness about PA, health care providers can augment the self-confidence of elderly individuals to begin exercise regimens [18].
Environmental factors
A lack of sports facilities was considered to be an especially important barrier. In this regard, construction of playgrounds, sidewalks, parks, or other fitness facilities could motivate individuals to participate in exercise, such as walking. Governments play an important role in providing subsidies and funding for health facilities, such as health centers and walking paths [2]. It was found that a lack of adequate facilities in organizational settings led to a decrease in enthusiasm for PA [52]. Likewise, in Iran, a study confirmed that the presence of exercise facilities, parks, and walking or cycling routes increased elderly individuals’ motivation to engage in PA [16].
Some studies have shown that the availability of a resting place, such as benches along walking paths, may facilitate walking among the elderly. In this regard, for the elderly, it is very important to ensure easy access to safe, beautiful, and interesting places for walking. For these reasons, the elderly were found to prefer routes with places for them to rest [25].
The weather, season, and temperature were identified as potential barriers. Nadri et al. [16], in Iran, reported that participants considered an inappropriate environment to be a barrier. In addition, other studies have shown relationships between natural changes (season, weather, and temperature) and the intensity of PA [25]. In general, more intense PA was observed in the spring (40.1%), in sunny weather (76.8%), and at moderate temperatures (56.2%). Elderly individuals were found to engage in more frequent walking in sunny weather than in rainy weather, and their walking rate was higher at temperatures below 60°F than at high temperatures (81°F). Schmidt et al. [53] reported that “unpleasant weather” such as cold, snow, and extreme heat was a barrier. In addition, a study confirmed that the weather was a potential barrier for the oldest old people [4].
It is worth mentioning that we found some similar barriers and motivators. In some reviewed studies, a link was found between the benefits of prayer and PA. The energy cost of Muslim daily prayers was about 80 calories per day, implying that daily prayers could be considered a form of PA [12,54].
There are two important implications of these findings. First, the factors identified as important herein should be analyzed with regard to gender. Second, it is necessary to consider geographical areas and the accessibility of facilities. Additionally, the type of intervention program (community- or individual-based) is an especially important factor for encouraging the elderly to participate in exercise.
This systematic review has the following limitations. First, no information was extracted on differences between men and women. Therefore, further research is needed to identify any such potential differences. Second, it is possible that differences existed among participants and authors in the definition of exercise and PA. Third, most studies were conducted in developed countries, which may have yielded country-specific results and decreased the generalizability of the findings. As a final limitation, due to inconsistencies and heterogeneity in the data gathering and analysis methods used in the quantitative articles, it was not feasible to conduct a meta-analysis.
CONCLUSION
This study presents a comprehensive literature review and analysis on the barriers and motivators to PA in the elderly. Most barriers involved the intrapersonal and interpersonal domains. According to the population composition of the countries that were analyzed—especially Iran—interventions to address this issue are essential. In addition, the elderly may have different perceptions of barriers and motivators that need to be considered.
SUPPLEMENTARY MATERIALS
Supplementary material is available at http://www.e-epih.org/.
epih-41-e2019049-suppl.docxNotes
The authors have no conflicts of interest to declare for this study.
AUTHOR CONTRIBUTIONS
Conceptualization: SY, AR. Data curation: SY, HMS. Formal analysis: SY, HMS, MG. Funding acquisition: SY, AR, HMS. Methodology: SY, AR, HMS, MG. Project administration: SY, AR. Visualization: SY. Writing – original draft: SY, HMS, MG, AR. Writing – review & editing: SY, HMS.
Acknowledgements
This study is related to project No. 1396/56458 from the Student Research Committee, Shahid Beheshti University of Medical Sciences, Tehran, Iran. We would also like to express our appreciation of the Student Research Committee and Research and Technology Chancellor of Shahid Beheshti University of Medical Sciences for their financial support of this study.